

This post from Dr Alan Garner tackles a core problem for all practitioners who give a damn – how do you know you’re doing it well? A chat worth having and Alan has a pretty good summary of the Carebundle approach.
How do we measure quality in prehospital and retrieval medicine? Speed? Number of procedures performed? Number of twitter followers?
Seriously though, this is a question that vexed me for many years as a service director and trying to find metrics that measure things that mattered seemed an elusive task. The major part of the problem stemmed from the heterogeneity of the patient population that we treat. Even simple (but easily measured and therefore attractive to bean counters) things like timeliness are not straightforward. Not because they are hard to measure but because sometimes time matters and other times it very clearly does not. Indeed emphasising it as a measure could lead to perverse outcomes for some patients.
Let me give you a couple of examples to illustrate the problem:
Case 1. Central abdominal stab wound with hypotension.
There is almost no prehospital intervention that matters in this patient except gasoline and perhaps tranexamic acid. I don’t think anyone would argue that time is a reasonable quality measure in this patient.
Case 2. COPD patient in a small hospital an hour flying time from the nearest intensive care unit.
Patient is eventually stabilised on non-invasive ventilation after three hours of effort by the transport team at the referring site. They are then safely transported. Clearly for this patient time does not matter at all. Reporting turnaround time at the referring site in this patient may place subtle pressure on the team to intubate the patient early and depart – a move that is very clearly not in the patient’s best interests and would have placed the patient at significantly increased risk of unnecessary morbidity and mortality.
This got me thinking that our measures of quality had to be disease process specific or we were never going to move forward. Speaking with Erwin Stolpe was the turning point in my thinking.
You Should Really Try to Know Erwin
Many of you will not have heard of Erwin. Sometimes when I talk to people or read things on social media I get the impression that physician staffed HEMS started in about 2005. The reality of course is quite different. Erwin is a trauma surgeon from Munich who began flying as a resident on the Christoph 1 service out of that city in 1968 (yes, not a typo – 1968).

These days he no longer flies but is chair of the ADAC medical committee. For those unfamiliar with ADAC they run about 35 physician staffed HEMS bases in Germany and also operate several jets for longer range transports. Their HEMS services alone conduct about 50,000 prehospital cases annually. The breadth and depth of experience of this organisation is extraordinary and Erwin has been there from the beginning. You would think there might by a few pearls of wisdom there and you would be right.
The Key Cases
Erwin described to me the “tracer diagnosis” process they use to track the quality of the care that they provide. Analysis of their prehospital caseload indicated that four diagnoses made up 75% of the cases they attended. For these four diagnoses they defined the treatments that they expected the teams to achieve (see pages 52 onwards of this presentation by Erwin for more detail). They used national and international consensus guidelines as a base. They then began reporting against those criteria and they have also started to publish that performance.
What Erwin was calling “tracer diagnoses” is probably better known to us in the English speaking worlds as a “Carebundle”. Lots of people will be familiar with the ventilator Carebundle for intubated patients in the intensive care unit. Adherence to the items in the bundle is associated with lower rates of ventilator associated pneumonia. In NSW and Queensland, Health Departments have introduced bundles for central line insertion in order to tackle the rates of central line associated bacteraemia. In this case the bundle applies to a procedure or process rather than a diagnosis. Is there a place for this kind of methodology in the prehospital and retrieval world to improve quality too?
What are we talking about when it comes to PHARM?
Let’s start by looking at what a Carebundle is.
“A bundle is a structured way of improving the processes of care and patient outcomes: a small, straightforward set of evidence-based practices — generally three to five — that, when performed collectively and reliably, have been proven to improve patient outcomes.”
This definition is taken straight from the Institute for Healthcare Improvement (IHI) website. There is a bit of controversy regarding whether the items in a Carebundle really need to all be completed for the bundle to be effective in some sort of synergistic way or whether they are in fact just a checklist of items that have been shown to be effective and you get as many done as you can. I am not aware of any evidence for the synergistic effect multiplier that is implied on IHI website. I think it is unarguable however that you should try and get as many of the things that are proven to make a difference to that condition completed as possible. That is certainly the approach that we have taken.
Another quote from the IHI website describes for me what we are trying to achieve by using bundles:
“The power of a bundle comes from the body of science behind it and the method of execution: with complete consistency. It’s not that the changes in a bundle are new; they’re well established best practices, but they’re often not performed uniformly, making treatment unreliable, at times idiosyncratic. A bundle ties the changes together into a package of interventions that people know must be followed for every patient, every single time.”
Using Carebundles in hospitals is clearly not new. Even in EMS it has been previously described for benchmarking purposes. The attraction of the methodology for me was that we would know if our care for patients with severe head injury for example was following the best available evidence and we would know what proportion of our patients were receiving that care. I did not want just some of our patients to get that care, I wanted all of them to get every item of care that we could identify matters for that disease process all of the time.
Making it Match What We Do
For our rapid response service in Sydney we then determined from our medical database the diagnoses that cover 75% of our caseload as ADAC had done. For us this resulted in the following list:
- Multiple blunt trauma
- Isolated severe head injury (GCS<9)
- Burns (>15% BSA)
- Penetrating trauma
- Immersion/drowning
- Seizures (to which we were often being dispatched as they were mistaken for head injury or had caused a minor traumatic event)
- ROSC post primary cardiac arrest (similar to seizures – trivial traumatic injury and patient in VF)
- Traumatic cardiac arrest (for us this is the HOTTT Drill which I have described in a previous post, well podcast but which also includes the HOTTT Drill package to go with it).
We then turned to the evidence based consensus guidelines, Cochrane reviews and good quality RCTs to define the Carebundle items. This is a sobering process as you realise just how few interventions there are that have good evidence to back them up. This is particularly true for prehospital care where we are often operating in an evidence free zone. In many cases we had no choice but to go with the consensus (or best guess as I like to call it). We decided that we would include intubation for unconscious trauma patients for example despite the evidence not being all that strong and in many cases contradictory.
When we had defined the items for the specific diagnosis we printed them up on cards that team members carry in their pocket. These serve as a checklist which teams use on site or in transit just to be sure that they have covered all the items. Below is our isolated severe head injury card – the item I constantly forget is the blood glucose level (BSL). Highly embarrassing if this is low when you arrive at the trauma centre! I for one am glad to have the prompt.
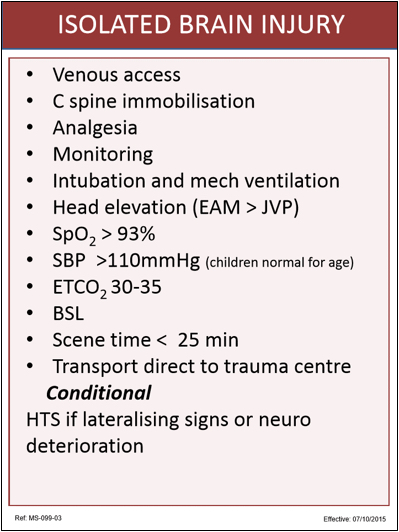
Some of these items are extrapolated from in-hospital care. For example having the external auditory meatus (EAM) above the JVP makes sense in terms of managing raised ICP but there is no direct prehospital evidence that shows this changes outcome. We have also set relatively conservative targets for things like oximetry and blood pressure. Most of the evidence suggests SpO2 >90% is enough but we felt that desaturation happens very rapidly from this point so we would rather aim a little higher.
Aspirations and Signals
Some of the items we knew from the outset that we would never achieve in all cases. Scene time of <25mins is the obvious example. When a patient is trapped this is outside of our control. We know however that one in five patients with a severe head injury will have a drainable haematoma that is time critical. We therefore included this item in order to signal to the team that we expect them to treat severe head injury as a time critical disease in the prehospital phase.
Some of the bundles have conditional items as well. For head injury this is the hypertonic saline which we only expect to be given if there are lateralising signs or neurological deterioration.
When the team returns to base they complete an audit form indicating if the bundle items were achieved and if not, the reason for the variance. This both reinforces for our personnel the contents of the bundles and also allows us to report on compliance. Below is an example of our report for severe head injuries showing the reasons of variance in the comments section.

You can see that we don’t meet all the targets all the time, and there is usually a good reason when we don’t. However the Carebundles allow us to be transparent about what we think good care is, and also about how successful we are in achieving it. We include Carebundle compliance (along with a lot of other stuff) in our external reporting in NSW to the Ministry of Health, NSW Ambulance, The NSW Institute of Trauma and Injury Management and all the trauma centres to which we transport patients. Transparency is a key component of good governance and this processes helps us to achieve that.
Those People Were Here First
The concept is not new. I merely walk behind the giants of the industry and follow their lead in this. It is also worth noting that Russell MacDonald from Ornge in Ontario is leading a similar project with an initial group of 10 “tracer diagnoses” amongst a small international collaboration of critical care transport providers. It will be interesting to see how closely their bundle items accord with our own. Aligning our bundle items would allow us to benchmark ourselves against similar organisations in other parts of the world and create opportunities for us to learn from organisations who manage specific conditions better than we do. In the end this is about maximising the outcomes for our patients and I will gladly accept any help I can get in achieving that.
Notes:
Here’s the stuff referred to along the way, because the originals remain a vital part of looking at the issue.
Here’s a link to the English version of the “tracer diagnosis” abstract.
(Well, not all of us are clever enough to know German.)
Here’s the direct link to the IHI page.
The image of Erwin Stolpe comes from the Intercongress flickr account and is unaltered under the CC 2.0 licence.

