
This is the written version of a talk by Dr Andrew Weatherall for the South African Society of Anesthesiologists Congress 2017, just held in Johannesburg. It’s probably just about the shiny things.
You probably figure that a talk on prehospital paediatric medicine in Sydney should be about shiny pictures of that thing we call the coat hanger. Or maybe actions shots of this character …

And of course there are a lot of cool things we can do in prehospital paediatric care. Maybe the best thing to do is to start with a story. It’s a story of a kid we’ll call B.
Lazy Mornings
One of the odd features of Sydney is that on its edges there are some areas that are essentially rural. They’d take an hour or so to drive to from the CBD, but are probably only 10-15 minutes flight from the base.
One day, a Monday I think, on one of the properties out that way there’s a Dad watching cartoons with a couple of his kids. They want to keep hanging out and he has a bit of work to do moving some earth so he heads out, kids parked firmly on the couch and closes the door behind him.
In the truck he starts to manoeuvre to turn it around. Back. Forward. Back with a glance at a side mirror and he sees legs. They look like the legs of his 4-year-old and they are sticking out from under the wheels.
I imagine the seconds it took to reach her felt like a long time. I imagine the wait for help to arrive felt a lot longer.
Things That Aren’t Common
The weird thing about being an Aussie talking about trauma in South Africa is that I am not talking about something that is common to us. Most of the audience would laugh at our numbers. The NSW Institute of Trauma and Injury Management published some stats from the 2015 annual review and across the whole of NSW there were 3970 major trauma patients. The busiest adult trauma centre would see a bit north of 600. Across the state the kids’ hospitals would see less than 200 severely injured kids between the three of them.
So I should pack up and stop talking I guess?
Well I guess the thing we could reflect on is that if you can’t rely on exposure to numbers to get everybody better and produce better outcomes there are other things you can focus on. You can start with the system to make the response bring the hospital to the patient quicker. It’s over an hours drive back once anyone gets there.
That day the NGO I spend time with was called about B and was airborne in minutes to get to her. This ability to get in the air quickly came from a trial to look at ways of getting care to patients quicker where every second that could be cut down was thrown in the bin.
The perpetual question we are asking is “what can we bring to the accident scene that will make things better?”

Change the Scene
Let’s imagine a different version for a minute. Let’s imagine in the perpetual construction site that seems to be outside most hospitals, this happened out the front door of where you work. What would you offer this kid?
My expectation is you’d rapidly assess for exsanguinating haemorrhage. You’d work as quickly as possible to ensure A, B and C are adequately sorted and you’d get analgesia on board. You’d image, transfuse if you need to, consider tranexamic acid and splint any fractures.
If oxygenation and ventilation means anaesthesia, intubation and ventilation (maybe even chest decompression) you’ll do that. You’ll assess and reassess as things evolve, operate where it’s really needed and keep making new plans to cope with a dynamic situation.
So here’s a question to consider – which one of these should we forget about while the patient travels by road for an hour to reach the front door of the hospital? If you’re the anaesthetist up in theatres who will meet them later, which ones do you not want to have been looked at early?
We can take almost anything we want to the scene. Helicopters carry stuff. So we take with us all the equipment for advanced airway management, a small ventilator and oxygen in our backpack. We can decompress chests. We can splint. We can ultrasound, tourniquet, pack wounds with haemostatic agents, give tranexamic acid and transfuse. We have to get there of course.
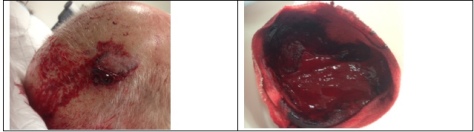
And on this day the team did. They were confronted with a child looking more than a bit pale and cool peripherally. Her HR was 140 and above with a brachial pulse palpable. Her GCS was 9/15. Her injuries were apparently below the umbilicus but looked like they included a fractured pelvis and right femur. She had been eviscerated and had a large skin flap extending from the front of the abdomen all the way around her back. She was still under the truck.
Over the next 50 minutes or so, the team obtained intraosseous then intravenous access. They performed a controlled rapid sequence intubation. They splinted fractures and covered up defects. They delivered warmed red cells. They got her to the hospital. She was fairly stable through the emergency department and then the operating theatres. She made it to PICU.
She made it home.
Cool story, huh? But also really irrelevant if you’re talking at a conference in a different health setting, right?
Another Change of Scene
What if this happened in Cape Town? Which team would turn up then. The dispatchers are likely not to have medical background. An activation of advanced teams will happen some time after the sent team gets there. The team that first arrives will have paramedics with variable levels of training. They might not be able to give a range of stronger analgesic agents. They will have more limited options for airway management. They are likely not to feel as comfortable with cannulation in kids as in adults.
The kid gets what they get.
The thing is, I could be describing the same back in Sydney. I gave you a story from the system on a good day. We know a system like that is there but we don’t really offer it. Most days our kids will get teams that finds kids really challenging (because they are of course).
Getting the Team There
How do I know this? Well we looked.
A while back CareFlight was running a randomised trial to try and activate advanced teams to patients on the basis of the initial information that gets called in using a strict protocol. The trial applied to adults but we were asked to offer it to kids as well.
The crew (doctor/paramedic/pilot/aircrew) next to the helicopter had access to the screens and took it in turns to match the high acuity calls to tasking criteria and even to call back for more info if required. A decision to get in the air, cross-checked with central coordination for kids) had to be made within about 5 minutes of the start of the call.
For a while the systems (crew watching and central coordination watching) operated alongside each other. So we had a look at how that worked out. Over a period of time where the Sydney area had 44 severely injured kids, on that initial info the advanced care crew picked up 20 of them. The central guys looking noticed 3.
The numbers are obviously small (not much trauma, remember) but when the crew were watching and going to jobs it also made differences to the system. As they always brought kids back to the kids’ trauma centre, the time to get there averaged 92 minutes. When they were not available (on another job or offline) that time became 296 minutes. That’s for a few reasons but in no small part to some of those patients getting taken to other hospitals and waiting for transfer.
So there’s one thing you can do for your more trained up teams without much infrastructure required to get the right team there.
And I hope someone picks it up because in Sydney they abandoned it. At the end of the trial the screens went.
Another Look
So we had another look to see if the system had picked up the slack. We looked at the time when the advanced crew had the screens and the time after that. These were longer time periods (34 months in the first epoch and 54 months after which equated to 71 severely injured kids before and 126 after).
In the first 34 months the collaborative system picked up 62% of those severely injured kids and the average time to hospital was 69 minutes. In that latter period, with centralised looking alone, 31% of kids were triaged to advanced care, the version of care the system says it wants. The time to reach the kids’ hospital averaged 97 minutes.
You can imagine that this is something I find … disappointing.
But you might also be thinking “If you are suggesting I try and change a whole system then you are an extremely crazy person affected by anaesthetic gases that have rotted your brain because that will involve meetings, and talking to people who do politics and some of those people will expect me to wear ties and that is not why I got into anaesthesia”.
And that is fair.
But a much as I’d love us to do things about systems there’s something we could all focus on right now to try and make a difference.
If the system is mostly going to send the “not pointy end” part of the system, then we should also look at the care most of the kids will receive.
The Big Story
Every talk on prehospital stuff by a doctor can end up being mostly about the really sharp edge. But in NSW less than 1 in 5 kids ever see the advanced care team. So the biggest bang for our buck is in making sure all the kids get access to prehospital clinicians who feel confident working with kids and give them what they need on indication, not influenced by age alone.
When we focus on the pointy end the chances for gains are pretty marginal. Let’s look at intubation for example. Advanced EMS practitioners in Switzerland have published on their efforts and the highly trained and experienced professionals mostly get the tube in without incident but almost 1 in 5 kids had the wrong-sized tube and the majority were placed too far down the airway. Bringing up the whole of the prehospital provider group to a level above Swiss advanced EMS is probably a pretty big effort.
Particularly when you look at stats like those from Prekker et al looking at a big EMS system in Washington where intubation was an option. A paeds response happens for them in 1 in 2198 callouts (there were 299 in total in 6 years spread across all the practitioners). Their first pass success was 66% (though they did eventually get there in 97%) and 10% of the patients needing intubation needed 3 or more attempts.
And I can’t tell you what the oxygenation was like through that and really oxygenation is the name of the game.
The simple truth is kids get a raw deal at the pointy end. Everyone finds them tougher. Bankole et al compared kids receiving high level EMS care around New Jersey with a severe traumatic brain injury and compared them to the adults being looked after by the same really well trained first responders.
20% of kids with a GCS under 8 had no attempt at airway intervention. Of those intubated 69.2% had complications and 29% (vs 2.27% in adults) had a failed intubation. Even cannulas were placed in only 65.7% vs 85.9%.
It starts making you think that if those of us in prehospital medicine looked harder at the thing we want to achieve, oxygenation, rather than interventions that sometimes can do that but have big potential complications we might be able to change things for a bigger population of kids.
Recalibration
Although there are problems drawing on battleground experience in civilian trauma care, particularly in kids, there is a quite interesting paper from Sokol et al. looking at the Camp Bastion experience with 766 kids with traumatic injuries. 20% of them needing some sort of intervention and circulation measures (particularly stopping bleeding) was the most effective. Simple airway manoeuvres were done not often enough and interventions for breathing (like chest decompression) were a lesser order issue than circulation issues.
So perhaps what we should focus are things we could train more people in and more prehospital providers of all experiences could deliver:
- Recognising the sick kid.
- Stopping haemorrhage effectively.
- Assessing A and B and delivering effective bag-mask ventilation.
- Cannulation and appropriate fluid use.
Recently we’ve done some focus group work at The Children’s Hospital at Westmead with clinicians who do paediatric airway management and one of the strong themes emerging as we write up is that all of them rate airway assessment and bag-mask ventilation as the most vital skill they want to be good at and they’d like to pass on.
There are all sorts of interesting hints here. Hansen et al conducted an exploratory study in 2016 to look at how well paramedics recognised and treated in croup. After whittling through records their small study looked at 14 patients with a primary upper airway issue. 8 of the patients had “stridor” or “croup” explicitly noted in the tasking or information noted by the responding paramedics. 6 had trigger words like “barky cough” or something pretty convincing. All of them received salbutamol, not the nebulised adrenaline or other treatments on offer.
But Some Things are Easy, Right?
Analgesia though, that might be an easier target because relieving pain in kid sis a no brainer.
Well, no.
Samuel et al. published a systematic review of evidence looking at analgesia provided by prehospital providers for kids in 2015. In it they describe a review of 55642 patients where 26% of the kids had trauma and another 16.1% of kids had a primary complaint with significant pain.
0.3% of the kids were given any analgesia.
There were other studies included reporting rates of analgesia administration for fractures of 2.1-3.2% (and at least one with 0% in the under 5s with fractures).
What is going on?
Well sometimes there might be limitations in what the paramedics have available (e.g. opioids or not, ketamine etc). One physician system showed 92% getting given strong analgesia in these sorts of patient groups.
There may be a fear of drug errors because there is work suggesting issues with drug dosing in kids in more than 30% of prehospital cases.
However Rahman et al have also done work exploring the perceptions of paramedics in providing analgesia to kids and showed very high levels of reported discomfort with providing and assessing analgesia in kids. More alarmingly 25% of respondents indicated that kids needed less analgesia because of immature nervous systems.
These are not small chips either. Schreier et al looked at PTSD symptoms after just mild to moderate trauma (things like isolated fractures) in kids. At 18 months (in an admittedly small study) 38% of the kids they looked at had at least mild symptoms.
PTSD in kids expresses itself as poor attendance at school, missed marks in education and social disengagement.
While < 4% of kids are getting analgesia for obviously painful things, there are things we can tackle that don’t need a rapid sequence intubation and a snorkel.
What is the cost?
So the cost to patients will undoubtedly be big if we are sending teams who don’t feel comfortable in kids, but is the cost of addressing it prohibitive.
I reckon not. Here’s one example.
CareFlight, that little charity I mentioned, has started to treat education of first responders as a way of providing service to the community. By taking simulation education and courses mobile to rural and remote first responders maybe we can make the first person who turns up to the injured just that little more comfortable that there are things they can do.

Since 2011 they’ve reached almost every state in Australia and trained more than 3000 people. Participants don’t pay.
In the Western Cape there is an EFAR program that would be worth checking out that is seeking to enhance the response of first-aid responders.
But if you’re an anaesthetist or other critical care provider, then there would have to be ways for you to link up with local prehospital services and offer to help paramedics gain skills and experience.
Everyone in the room (or reading this) can probably provide analgesia. Everyone has seen a sick kid. Everyone knows how to splint and work on stopping bleeding. In particular I am full of a room of people who have exquisite skills in things we think of as basic, like bag-mask ventilation, but could be the difference between a patient being oxygenated on the drive in, or obstructed the whole way.
The Wish List
If you’re the anaesthetist waiting in that operating theatre when an injured kid is on the way, what’s on your wish list?
Mine would include the patient being identified and getting to me as quickly as possible. I’d hope the team that reaches the patient can recognise if they’re sick and keep reassessing well. I’d hope they felt confident managing the airway and could optimise oxygenation as much as their skills allowed. I’d love it if they turned up with some form of intravascular access and some analgesia on board.
The priorities to start making that happen for more patients is actually not about BIF with the noisy rotors. The priorities are the same if you’re looking at an old bridge across a harbour. Or some mountain near the sea.

Or a downtown area closer to the sky.

Notes:
I cannot express the depth of my gratitude to the patient and family who have granted permission for the use of their story as part of education in this area.
Thanks also to the clinicians involved in the case, Dr Rob Bartolacci and Ben Southers, super paramedic, for background on their case and the shot from the sky that day.
A huge thanks also to the brilliant Jo Park-Ross, Flight Paramedic from AMS in Cape Town and Ross Hoffmeyr, an anaesthetist also working in this area down in Cape Town for helping me understand more about the local system and checking my work.
A shout out too to Colin Brown and Greg Brown (no relation) at CareFlight for the stuff about the MediSim program.
As part of the invited faculty the organising committee covered travel, accommodation and registration for the conference.
The images of BIF and Sydney are from my personal collection. Other images are from the Creative Commons area of flickr and are unmodified here. Paul Saad posted the shot of Johannesburg and the shot of Cape Town is by Damien du Toit.
Right, now the things to read…
Here are the trauma stats in NSW for 2015:
Here is the Head Injury Retrieval Trial:
Here are the tasking studies:
The Swiss study:
The thing by Prekker et al.:
And the first responder TBI comparison:
Here’s the battlefield stuff:
The thing on assessment and treatment of upper airway obstruction by paramedics, which is exploratory but interesting is here:
Now here’s that analgesia review that is a sobering read:
Here’s the thing about comfort level of paramedics in providing analgesia to kids:
Plus that little PTSD study:
If you wanted to get a little more info on that mobile simulation training CareFlight do here’s a link.








![Getting to a CT scanner in a more timely fashion than this was a way of tracking patient progress through their care. [via telegraph.co.uk]](https://careflightcollective.com/wp-content/uploads/2015/03/mummy-copy.jpg)
