Sometimes the really basic stuff needs better coverage. This series will probably start popping up a bit because sometimes it’s good to get people to share the stuff they wish someone said at the start. Here’s Greg Brown with simple techniques that could make all the difference that we should definitely do well.
Here are two sayings you hear all the time:
“Simple measures are lifesaving”;
“I thought it was common knowledge”.
More and more we are discovering that only one of these sayings is true. Yes, some of the simplest clinical interventions are the highest yield, but there is nothing common about knowledge. Why is it then we don’t often talk about or pass on these lifesaving skills and knowledge? A lot of the time we all put it down to “if I know then everyone knows”.
So it is about time that we all started talking about these simple and or basic interventions that save lives (or at least minimise the mess we have to clean up at a later stage).
In this the first of an indefinite series titled “I wish I knew then what I know now” we will be looking at the simple yet effective tips and tricks that either:
We wish somebody had taught us at Uni / college;
Didn’t exist then but do now; or, (c)
We are at risk of forgetting due to an abundance of modern technology.
So quieten the voice inside your head that is saying “I am a senior doctor / nurse / paramedic / rescue guru – what could I possibly learn about the basics?” and take up the challenge to continue reading and see if you know our little tips and tricks. Or maybe you’ll have some tips and tricks to send back our way. With any luck these posts will generate some healthy continuous improvement and discussions all about the patient. We might all be surprised what we’ll learn along the way.
Controlling the Red Tide
This is not a post about quelling a Communist insurgency. Basic haemorrhage control appears to be a dying art (no pun intended). The skill of haemorrhage control is used across all areas of healthcare whether you work as an immediate responder in the pre-hospital environment, as a paramedic or professional pre-hospital care provider, within an emergency department, ICU or wards of a hospital or simply as a relative or friend after hours.
However, our observations of many of the health care professionals and volunteers that we work with (or teach) indicate that the basics are not known and rarely taught these days. So let’s look at some – direct pressure and indirect pressure.
Direct Pressure
Direct pressure….it sounds simple enough, but how do you achieve this? Let’s use a simple laceration to a limb with venous bleeding as an example.
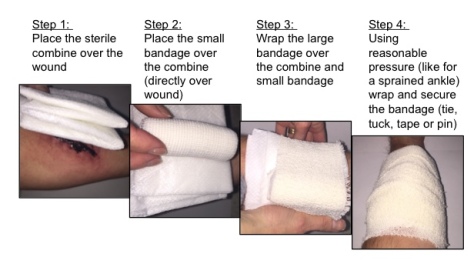
The standard approach to applying direct pressure will see many people reaching for a flat combine (or other blood soaky-uppy type device), placing that directly onto the wound and bandage away. What about when that bleeds through? Simple – repeat step 1 by applying a second combine on top and bandage away. What about when it bleeds through again? Easy – repeat as above. Right? Well, maybe not so much.
The problem with this process (that we have all been taught at some point) is that at no stage are you actually applying direct pressure to what is bleeding. This is not a criticism of the individual – rather, it’s a firm clue that perhaps there is an issue with the teaching.
To explain what is going wrong we ask you to consider a leaking garden hose. If your hose has a small leak in it, what happens if you place the palm of your hand down on the leak? The water oozes out underneath your hand – this is just like the flat combine being placed onto a bleeding wound (i.e. the blood leaks out the side).
Now, what if you were to walk up to your leaking garden hose and place a single finger on the hole – what would happen? Well, assuming that there is not massive pressure behind the leak then the leaking water would cease.
This is direct pressure in action. One needs to think about what it is you are actually trying to achieve with your bandaging technique – flat on flat with distributive pressure is different to direct pressure. You need to add a pressure device, and a simple solution is to add a small rolled up bandage on top of the first combine – placed directly over the source of bleeding – then bandage over that.
These images describe this as simply as we can (it’s much easier to demonstrate than describe):
So simple to achieve when you think about it, and also very cost-effective.
Now, there are also various commercially made bandages out there that achieve the same thing. Two that are widely used across our planet (well, certainly in Australia…) are “The Emergency Bandage” (aka Israeli Dressing, made by FirstCare) and the OLEAS Modular Bandage (made by Tactical Medical Solutions). If you have the ability to have these as part of your kit then these are great additions – they also do a lot more than just apply direct pressure, but that is a story for another day.
Remember though, big and flashy is not always needed to be effective. The main thing to remember with direct pressure is that smaller in this case is better. By this we mean that if you only need finger point pressure to stop the bleeding don’t use a combine as your patient will bleed more than they should; and let’s face it – once the blood has left the body it is damn hard to put it back.
Story Time
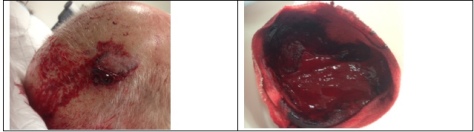
Many years ago I was working in a small(ish) country hospital when an elderly gentleman was brought in by ambulance. This gent had slipped on a wet pavement and unfortunately hit his head on the sidewalk whereupon he commenced bleeding from a nasty scalp wound.
A first aider from a nearby shop applied standard level treatment – flat combine and a crepe bandage. The ambulance team arrived shortly thereafter and, noting that the first layer was soaked through with blood, applied a second combine and crepe bandage then commenced transport to hospital. Believe it or not, the process was again repeated when the second layer had bled through – that’s three combines and three crepe bandages.
And yes, I’ve previously got clearance to use these photos.
In the hospital the man’s dressings were removed and he was still bleeding from the wound. A single gloved finger was used to apply direct pressure and, lo and behold, three minutes later he had stopped bleeding.
One of the hospital staff then weighed the combined soiled dressings – the clot, combines and bandages weighed in at just under 800g. That is a LOT of blood what would have been better served remaining in the gentleman’s circulatory system.
Indirect Pressure
Indirect pressure is a great intervention that will stop (or at least slow) bleeding while we implement effective wound treatment. By this we mean you need to stop the blood spilling onto the ground while you apply the arterial tourniquet or pack the wound.
Indirect pressure is achieved by applying a compressive force proximal to the damaged artery until the bleeding stops (or is at least slowed down). There are in essence two methods of achieving this:
Use of manual indirect pressure (e.g. a knee to the groin (femoral artery) or fist / knee to the elbow (brachial artery)); and
Arterial tourniquets.
This Collective entry will only deal with the former; we’re keeping arterial tourniquets up our sleeve. Or somewhere.
So, manual indirect pressure.…again, it sounds simple enough. But how do you achieve this?
Many people are taught to simply apply some form of pressure to an artery above the wound. But, given that many first aid courses no longer teach the taking of pulses (for the international readers, within Australia a few years ago “first aid” seemed to become very cardiac arrest oriented, and we all know the presence or absence of a pulse no longer forms part of the CPR ritual for many people…) how can a first responder be relied upon to locate a brachial or femoral pulse in an exsanguinating patient when they’ve never been taught?
It is not just the first responders who are at risk here. As healthcare professionals we need to be able to act reliably and instinctively in the presence of life threatening haemorrhage. None us were born with ultrasound-guided vision (patent still pending so back off), and if you are reaching for your favourite POCUS device to find that vessel then you are doing your patient a great disservice.
The money shot is to go for the joint – at least here the pulses tend to be more superficial – and apply pressure there. How much pressure? Lots, in fact as much as you physically can! Manual indirect pressure requires a lot of force. To be most effective one needs to use as much of their own body weight as possible. Don’t stop here though – there is a vitally important extra step to this technique that is not widely known.
If all you do is apply a compressive force to the area in which the artery lays you stand a very good chance of missing your target’s location and sitting either left or right of where the artery actually lies. To ensure that the artery is compressed we recommend adding a twist of the knee or fist after compressing in order to kink off all vasculature under where the compressive force has been applied. We call this technique a “Z Lock”. This helps ensure that you are going to stop (or at least slow down) the bleeding and buy yourself time to treat the actual wound or apply an arterial tourniquet (if warranted).
Press and twist. It makes a difference. Also those are the instructions for that ultrasound-guided vision device. Damn. Shouldn’t have mentioned that.
Summary
Direct and indirect pressure are powerful interventions that help minimise a patient’s blood loss. They are however often forgotten about during both teaching and application stages as we become more and more task fixated. So we challenge you to make these steps part of your training regimes when talking about haemorrhage control. Practice them or, as one of our former instructors used to say, “don’t just be good at the basics – be awesome at them!”.
Last time Jodie Martin, Flight Nurse extraordinaire dropped by she shared one of our most popular posts ever. Jodie returns with a little on the Top End experience of sepsis.
Time for a look at some remote medicine again.
CareFlight provides the aeromedical service for the top half of the Northern Territory (NT) in Australia. The area covered by the service is the same size as France but has only 160,000 people. And less vineyards.
As 115,000 of this population are in Darwin which is serviced by road ambulance services this leaves CareFlight to provide services to about 45,000 people in very remote and widely scattered centres, most of which are small Indigenous communities. The catchment area has only two rural hospitals which are non-referral centres with care otherwise provided in remote health clinics. Even then not everyone lives close to a rural hospital or remote health clinic. Some rural folk still have to drive several hours or even a few days to any level of health care. Access to health care is a real challenge when someone becomes sick.
The Top End of the Northern Territory may be sparsely populated with 0.2 persons per square km, but it has the highest incidence of sepsis in Australia and five times higher rates than those recorded in the US and Europe 1,2. It has been suggested that one of the reasons for the high incidence of sepsis is related to the higher Indigenous population in the Top End 2. The incidence of sepsis requiring ICU admission in the Top End of the NT for Indigenous people is reported to be 4.7 per 1,000. In the non-Indigenous population there are 1.3 admissions per 1000 people. When compared to the rest of Australia, the rate of admission to an ICU for sepsis is 0.77 per 1,000 2 with national 28 day mortality rates of 32.4% 1.
The Top End – Not Just Popular with People
Human-invading bacteria and viruses love the warmth and moisture of the tropics. To make things even harder, the Top End has the highest rate in the world of melioidosis, a very nasty pathogen found in the wet tropics of Australia. Melioidosis has been classified as a Type B bioterrorism agent by the Centre for Disease Control in the US and kills up to 40% of infected patients often from rapidly fulminant disease. However most sepsis is of the more common garden variety, but still causes severe, life threatening illness.
A quick editorial note that we have done another story from the Top End and still it’s not about crocodiles. We apologise but it turns out there are other things up there trying to kill you.
When you add the challenges of distance and retrieval times, meeting targets for sepsis treatment which are time-based would seem an impossible task. Given this, we were keen to review the retrieval of septic shock patients in our service to see what the outcomes are like and whether we could improve the process. The results have just been published in the Air Medical Journal which you can find here.
The patients were sick. A third of patients required intubation and 89% required inotropes. Median mission time however was 6 hours and the longest case took 12 hours. Given the remoteness and time delays inherent in retrieval over such distances with a population known to have worse health outcomes, you would expect mortality to be high. Surprisingly however the 30 day mortality in this group of 69 patients, which are predominately Indigenous, was only 13%. This is lower than previous rates described for both sepsis in Australian Indigenous populations and for patients in Australian and New Zealand intensive care units.
That’s Excellent, But Why?
It is interesting to speculate on the possible reasons for such good outcomes. Reasons might include:
The relatively young age of the patients compared with many series. Perhaps the better physiological reserves of younger patients are still a key factor despite the higher rates of co-morbidities.
Early antibiotics – these are almost always given by the end of the referral call. Good clinical coordination has a role to play in this too.
Early aggressive fluid resuscitation – the median volume of crystalloid administered was 3L during the retrieval process.
Inotropes administered following fluid resuscitation occurred in the vast majority of patients.
Early referral – recognising when a patient is sick. This is something we’d like to gather more data on. We didn’t record how long a patient was in a remote health centre before a referral call was made, but we have a suspicion early referral might have played a part here.
It is also interesting to note the good outcomes that were achieved without invasive monitoring in approximately half the patients retrieved. Perhaps there are shades of the findings of the ARISE study here where fancy haemodynamic monitoring really did not seem to make much difference either – what matters in the retrieval context is early antibiotics, aggressive fluid resuscitation and early intubation when indicated.
We did not randomise patients to invasive versus non-invasive monitoring and it is possible that the sicker patients and those with longer transport times received the invasive version. But it is also possible that we get too hung up on this stuff and it is the basics that really matter whether you are in the city or a really remote health clinic.
The Wrap
The Australian Indigenous population have poorer health outcomes than the general community. Outcomes are even worse for those residing in remote areas than those in urban areas. In our small study it is pleasing to see such good outcomes despite remoteness and long retrieval times. Our young patient cohort recovered well considering how sick they were but what would be even better is preventing sepsis in the first instance. The incidence and burden of sepsis in young Indigenous people requires preventative strategies and appropriate and timely health care resources. Improving access to health care, improved housing and decreasing overcrowding, decreasing co-morbidities and decreasing rates of alcohol and tobacco use are hopefully just some of ways we can possibly decrease the incidence of sepsis and contribute to closing the gap.
Notes:
That croc with almost enough teeth came from flickr’s Creative Commons area and is unchanged from Jurgen Otto’s original post.
Here’s the link to the paper that’s just been published:
At the recent Student Paramedics Australasia International Conference 2016 held in Sydney, Dr Andrew Weatherall was given the topic of “things paramedics can do to produce better long-term outcomes after traumatic brain injury”. This is a version of that talk modified for the blog.
This topic, that someone else came up with, gets it.
So much of the time in prehospital medicine we focus on things we measure in the first hour or so. The stuff we do before we hit the doors of the hospital. That fairly bogus ‘golden hour’.
Those things matter. But the big picture of trauma care isn’t the first hour. It’s the rest of the patient’s life.
Everything we do in the prehospital setting is really about whether they get back to what they were dreaming of doing. It’s not up to us what those dreams are. Your patient might dream of playing big time sport. They might dream of creating the world’s great collection of corn chips that look like ex-Prime Ministers. They might want to fly on the first trip to Mars (and almost certainly die of cancer because everyone seems to be forgetting about deep space radiation). When we care for them we sort of have to want their dream to happen for them.
So on the days when I get to hang out with paramedics instead of getting paid by the government to wear pyjamas and give drugs to kids, this is the aim. And traumatic brain injury is worth looking after well.
We could dive into traumatic brain injury by starting with a bunch of graphs from a physiology text. Let’s dive into something to make it relevant.
The Scene
This is the scene we’ll be going to. You’ll end up looking mostly at the patient who was driving the SUV. It looks like they had an initial collision, rolled over and then nudged up against the hatch that was veering off the road. Emergency services have been called by a passing pharmacy student who has done a First Aid course. They tried shaking and shouting and got no response. They thought about feeling for a pulse and they’ve found one.
This patient is clearly one who might have a traumatic brain injury (TBI). They could end up as one of the patients with moderate or severe TBI who lead to a cost to the system of around $8.6 billion each year. That comes from a report prepared for the Victorian Neurotrauma Initiative released in 2009. It estimated that for 2008 Australia would have around 1400 in the moderate TBI group and 1000 in the severely injured group.
And each one of those people doesn’t get back to their planned life. Some of them end up needing help with simple things for their whole life.
So this is the job and the clock started 5 minutes ago. What should we focus on? Is it all about RSI? Is it about early TXA? Is about the sort of stuff you need an advanced medical team for?
Well that could be the basis of discussion but we should start with a reality check.
If you look at the NSW Institute of Trauma and Injury Management report of the 2014 trauma database stats, there were 3458 severely injured trauma patients. 66% of the patients had an injury to the head. 3 of the top 5 severe injuries were subdivisions of subdural haematomas.
Of those arriving straight to a trauma centre, 80.4% arrived in an ambulance (vs 12.6% in a helicopter).
Even allowing for some of those ambulances having an accompanying advanced prehospital team, I think this grouping of numbers says something pretty significant: the vast majority of “big” trauma patients will get their care from paramedics.
This also means that if we want to save the most brain cells we should focus on making sure the patients getting those transports have the best possible care that those paramedics’ training can make happen. That’s more important across the population than the advanced team’s contribution.
There is a separate chat to have some day about trying to get advanced teams to the jobs where they might really help or the best way to do pointy end stuff. That’s just not the focus for this particular bit.
It does brings us to the first key thing that trained paramedics can do to improve long-term neurological outcomes – be there.
The nature of their training and their ability to focus on getting the vital things done and get moving means that paramedics will invariably lift the standard of care of the patient when they turn up and do their job.
Now exactly what they should do we’ll get onto in a bit but there will only ever be a small number of meaningful interventions to do for the patient so it makes sense to get it done as efficiently as possible and get moving. And of course while neurosurgery is mostly not an urgent requirement, about 1 in 5 patients will need some form of early head-cutter work. That 20% of patients really want professionals who are trained to make things move.
So it might seem like there’s not much meat on just saying “be there”, but I think it’s worth noting as we go that the standard way professional paramedics go about their business represents a step up compared to what was managed in the past.
Now that you’re there …
Back to the patient. When you get there, the patient looks to be in their mid-30s, is making breathing efforts and there is some air moving but it is fairly noisy respiration. Initial peripheral saturations read at 85% and the measured blood pressure of 95 mmHg is somewhere near what you would have guessed by palpating the radial pulse. The patient’s GCS is 7, the pupils are equal and reactive. A quick glance suggests the right femur looks like it’s adopting a more meandering course than usual on the way down to the knee.
So what should our aim be for these patients? What targets do we have that are the best evidence-based ones available?
Somewhat disappointingly we don’t have that much evidence for discrete targets. What evidence there is hasn’t really shifted much over the last couple of decades. Most of the stuff we do leans heavily on a general understanding of physiology as much as firm numbers.
But let’s focus on the numbers we do have. They’re based mostly on retrospective looks at info from big data banks. And the number to remember is 90. That’s the breakpoint because:
90% saturations is around 60 mmHg pO2 and we know that patients who have a reading below that value have worse long-term neurological outcomes.
90 mmHg is the magic BP number for adults – a measurement below this is associated with worse outcomes.
And these markers kind of make sense. We often think about the primary injury already having happened when we get to the patient and focus on avoiding secondary injuries which we view as discrete and separate extra insults. Add new injuries and you make the outcome worse.
It’s probably more accurate to say that the primary injury evolves over a number of hours. In that traumatised brain there will be excitatory neurotransmitters looking to party way too much for the cells to recover. There will be inappropriate triggering of cell death. Calcium will be getting places it shouldn’t and generally grabbing onto cell elements it should leave alone. Each secondary injury ramps up processes like these as they continue to evolve. It’s one of those times all evidence-based practitioners need to try and stop evolution from being a thing.
There are a few other things worth keeping in mind:
The brain is pretty simple in its demands. It wants oxygen and nutrients delivered.
Things that make blood flow decrease aren’t good (remember that the injury itself is quite likely to drop blood flow well below normal).
Intracranial pressure that is high isn’t great. It compromises blood flow.
Oh, and it’s also worth mentioning that there aren’t many things inside the head that we influence the volume of prehospitally:
There’s the brain tissue (and the associated fluid that goes with it).
There’s blood. Blood can be inside vessels which gives us some scope to manipulate how much flow is occurring. Occasionally it will be outside vessels and the vast majority of times that patient will get their definitive care at the hands of a neurosurgeon.
There’s CSF (which we have less influence over).
So if our aims are basic do we have to wait for advanced techniques to try and reach this target? Of course not.
This brings us to the second important “thing that we can do right now” – be basic.
Consistent delivery of basic measures has the potential to save huge numbers of brain cells. It’s more meaningful than waiting to try and develop the infrastructure and expertise to get more people doing advanced things like RSI.
The perfect example is impact brain apnoea. This has really only been described in any detail fairly recently by Wilson et al but there are accounts throughout medical history and the animal literature that describes a phenomenon of subjects forgetting that whole breathing malarkey in the immediate aftermath of trauma.
The suggested treatment? Open the airway and support ventilation. Those simple steps are meaningful.
They’re meaningful for all patients with TBI too. Which is why it’s worth getting back to the simple message of “A-B-C” which some sage once told us was as easy as “1-2-3”. Simpler than the transition to adulthood from child stardom if you were that individual anyway.
So let’s work through those simple little letters.
1. How’s your “A” game?
Well, is it anarchy?
Failure to do the basic bit of airway well is one of the commonest issues we see when welcome people training at the kids’ hospital. It’s such an important foundation though. So ask yourself whether you do the basic version of “A” well. Is your jaw thrust good enough to get those bottom teeth in front of the top teeth? Do you reach for adjuncts like oropharyngeal or nasopharyngeal airways as an aid? Are you quick enough to move to a two hand technique?
Most importantly do you make sure that you create a good seal with your mask? The value of a good seal is actually highlighted by work looking at pre oxygenation techniques. A colleague from CareFlight, Dr Chris Groombridge, did a nifty study with volunteers evaluating the maximum expired oxygen level you could achieve with different techniques. Anaesthetic circuit vs bag-valve mask (either alone or with nasal cannulae or PEEP valve or both) vs non-rebreather mask (with and without nasal cannulae).
And at the end of 3 minutes you still couldn’t beat either the anaesthetic circuit or the bag-valve mask with a well-maintained seal.
Hayes-Bradley et al did some work with a slightly different focus, evaluating the impact of nasal cannulae on pre-oxygenation with a bag-valve mask set-up or non-rebreather. Nasal cannulae helped only where there was a deliberately created leak in the seal.
Now you could take the line that it’s just pragmatic to assume you’ll end up with a leak. But why should we accept doing the technique anyway other than perfectly? Let’s focus on getting the seal right.
We’ve really taken that to heart at work, making the effort to maintain that seal throughout pre-oxygenation. It’s all part of ensuring that our focus on is on the main game – maximising oxygenation throughout the RSI rather than pushing on to the laryngoscopy and intubation step without optimising things up front. The brain wants oxygen more than it wants laryngoscopy.
That some prioritisation of the basic step of managing “A” well – perfect performance of basic airway manoeuvres, suction and use of adjuncts – can apply to all of us, whether we intubate or not. It’s the first step to delivering on our first aim – get those peripheral saturations above 90.
It also feeds seamlessly onto …
“How good are your “B” moves?”
Is it carnival material?
What about those patients who need support for the breathing part of the equation. That might be via that bag-valve mask set-up or you might have supraglottic airways as an option you’ve been trained to use.
The question here is not just how well do you do it but do you take steps to make sure you’re using that skill set in the best interests of the patient?
So if you think a supraglottic airway might be appropriate for a patient do you quickly assess if they’re ready for it with a firm jaw thrust and a deep suction before placing it? Do you check what the seal is like once it’s in?
And how do you measure your effort with the bag you hook up to that SGA? Because it’s easy to puff away like your hand is a talking sock puppet. We should really all be hooking up capnography wherever we can (for bag-valve mask work too). It might not provide a trace like the intubated patient but it will be more accurate than a guesstimate. And without having a sense of where you’re at with the CO2, how do you know if you’re not creating hypocapnoea when hypocapnoea is associated with reduced cerebral blood flow (and of course hypercapnoea could cause raised ICP)?
Doing the “basics” well requires a bit of attention. Who knew?
But you might well say, what about RSI? Shouldn’t we be figuring out how to train people to do that? Well while there is a probable role for RSI it is really hard to demonstrate the positive benefit. That is probably partly because prospective research in prehospital medicine is very hard. But the evolution of the research that’s out there suggests that getting that high stakes procedure done well enough to have the benefit outweigh the potential complications will take a very long and concerted effort.
Take for example just 3 studies:
The San Diego RSI paper – this suggested worse outcomes but subsequent analysis revealed performance of the procedure with significant periods of hypoxia (57% of those analysed had a desaturation with an average time of 160 seconds and a median fall in saturations of 22%).
HIRT – which took long enough in recruitment that the system changed all around it, rendering it very difficult to keep arms of the study in their planned arms. Those that received the advanced interventions team as intended did have a 14% reduction in mortality but it’s not robust enough to bank your house on.
The Victorian paramedic RSI paper – this showed benefit but there were more patients in the control group lost to follow-up and you’d think that those who did better would be the ones you’d lose. Just one different outcome in the control group would have made the findings insignificant. So it’s not robust enough but for different reasons.
So RSI makes physiological sense and most would still say it has a role. But it’s hard to make it pay off. We can all do the basics right every day from today.
What should we see when people are doing “C”?
It’s not like there’s some study out there saying “this particular prehospital intervention related to circulation and haemorrhage leads to better TBI outcomes” but we can focus on maintaining that blood pressure above 90 mmHg. So things that cause catastrophic hypotension (say, pneumothorax with haemodynamic consequences) need treatment with whatever the provider is trained for.
If there is external haemorrhage that has to be controlled so we can focus on doing that particularly excellently. If you’re putting on a tourniquet, think about providing proximal occlusion of flow first with your whole weight (e.g. a knee not just into the groin but leaning in and twisting a bit to really slow down flow before the tourniquet goes on). Really provide pressure to stop bleeding if pressure is the treatment you’ve chosen. Splint that femoral fracture to reduce loss of blood volume.
At the same time it’s worth noting that some of the evidence base for things we do is less strong than we might assume. As covered by Dr Alan Garner in the series starting here, the evidence base for pelvic splints improving haemodynamics isn’t based on huge reams of work.
Other options will probably come through for lots of practitioners soon. Haemostatic dressings or granules are likely to make a difference for some patients. With a little more evidence TXA might roll out across the land. And while there are very interesting concepts like prehospital REBOA out there to be wielded by a select few, something like the Abdominal Aortic Junctional Tourniquet might be a far more significant option on a population level. Judicious use in the exsanguinating patient with due regard to the potential downsides (particularly if it might take a while to get to somewhere else) could be an option for an awful lot more practitioners.
The Other Simple Things
That’s not the end of the simple things of course. Think about whether you can sit your patient up to drop the ICP. Is there a better way to maintain C-spine stability then a rigid collar? Is there anything constricting the neck?
Add a lot of simple steps together and you have pretty comprehensive efforts for those brain cells that just want blood to flow and nutrients to turn up.
The Group Who Doesn’t Get the Simple Things
And while we’re at it, there is one group who tend to get much less of all of the things, including the basics.
Kids.
Which is not great if you’re trying to think about how to provide better long-term outcomes. Their long-term is even more long-term.
Bankole et al provide just one example of a study demonstrating this. They looked at prehospital care around a New Jersey centre and compared the care received by kids with TBI to that received by adults. The numbers are pretty stark (though some of the headline items relate to interventions like intubation).
69.2% of the kids intubated had complications at intubation. 20% of kids with a GCS under 8 had no attempt at intubation. Failed intubation rates were 29.03% (vs 2.27% in adults). Kids also had higher rates of the dislodgement, oesophageal intubation, wrong size of tube choice and a requirement for multiple attempts.
Even intravenous access was placed less (adults had a prehospital cannula 85.9% of the time whereas in kids with the same spectrum of pretty severe injuries it was 65.7%).
More recently advanced practitioners in Switzerland published around the topic of advanced airway management in kids and while they did well initially, wrong tube sizes and wrong depth of the tube turned up again.
There are lots of reasons we do less well with kids. We see them less for a start and there can be additional scene distractions. But ultimately we need to recognise this and figure out a way to make sure we step up to the mark.
Back to the Scene
The patient has been making respiratory efforts but you can see the chest see-sawing a bit with diaphragmatic effort with an added breathing buzzsaw soundtrack. You jaw thrust and the airway improves. A suction improves the airway still further. You add a bag-mask set-up and really focus on a great seal. The saturations rise above 95%. The femur looks like it’s taking a meandering the scenic route towards the knee but it’s soon splinted and a big wound in the calf gets pressure to slow the bleeding. You’re on your way…
Now that sounds pretty easy. When you’re in a lecture theatre or reading a lesser known blog it sounds even easier. But we all know that the scene isn’t actually that easy. We’re assailed by all sorts of things and there is plenty of work in simulation sessions (like here) showing that when faced with high stress situations we tend to omit things we ordinarily wouldn’t, do things we’d normally not contemplate and remember all of it less.
This touches on the next thing prehospital practitioners have to do to provide better care for the brain – be the same with your care, everywhere. (The astute reader will notice that not only did I match the formatting to the other “be” statements, I made it internally rhyme. I’m really trying to make it seem meaningful.)
Beyond starting by acknowledging the risks of a deterioration in performance depending on the day or the job or the other stuff in our lives, we have to figure out how to be consistently excellent with our care. That’s what the patient expects. Their brain cells aren’t very interested in your back story or your motivation. They’d like you to do your job.
The strategies to try and make sure you always step up are way too many to go in right here, so it’s worth looking around. But use the team, communicate well, share your plans with those around you, use checklists or practice tactical breathing or other focus techniques or whatever it is that works for your good self.
Just don’t accept that you have to be a hostage to all those other factors.
And part of not accepting the status quo is striving to always provide better than we can do right now. That requires all of us to be a leader.
If we want to be able to provide capnography for all those patients whose A and B we’re managing then we might need to advocate for that. If we want to be able to look back in detail at how well we did, then monitors that only store information every 2 minutes (which is so often the case with prehospital monitors) aren’t up to scratch and we need to lead those demands. We need to provide leadership in governance and education to keep our standards constantly improving. We might even need to advocate solutions to issues in other areas of health that would free up paramedics to be out on the roads so they can work on that being there bit.
Future Dreams
While this topic is mostly about what we can do right now we obviously have to keep an eye out for what comes next. And I could well be wrong but my guess is that the thing that comes next that makes a big difference across the population to those who suffer a TBI won’t be one of the magic bullets being tried like progesterone, or EPO, or even TXA.
What would be really great is to actually know what the brain wants right now. Is the blood pressure of 100 mmHg actually adequate for this person’s brain or are they usually hypertensive and critical cerebral ischaemia is being added to your mix?
Does this patient actually need their CO2 a little higher than you might have thought because blood flow isn’t so great? Is their evidence of haematoma developing on one side that hasn’t shown up clinically?
That’s part of why we’re researching tech like near-infrared spectroscopy tissue oximetry. Now I’m not convinced that particular technology will provide that information reliably enough, but I do think that the most meaningful thing we could add to prehospital TBI care is more info about what this patient’s individual brain would like, rather than being stuck with population-based gross numbers.
And if we find that device the ultimate result will probably be that it tells us how to do the basics just that little bit better for this particular patient.
Because they might have big plans for corn chips that look like ex-Prime Ministers.
Notes:
OK, this was a really long post, but when you put a talk into post form it can be like that.
Here are just a few things from along the way you might like to go and look at.
Oh, and I put stuff over on the blog site at www.songsorstories.com relating to kids anaesthesia. If you look at the categories “airway” and “tips and tricks” and “cannulation” you’ll find some basic tips for working on things.
All the images here are from flickr creative commons and unaltered.
Did you scroll this far? Well you will inherit the earth that is constructed where scrolling is rewarded. Here, have this porcupine reviewing pumpkins as payback.