Well everyone else is doing the “look back, look forward” thing, so why not us as well?
It’s that time of year. You know, the one where we just want a few more days to kick back and relax or enjoy a southern hemisphere summer. What better way to look busy than a review of the posts that got the hits in 2017? Ssshhh. There may well be better ways but this is what we’re going with.
First up, music for the ears
Podcasts. People do them and people listen to them. Clever people do them regularly. We are not that clever it seems. We did finally get around to putting up a couple this year though and the most recent one was very comfortably the most popular podcast we’ve done. OK, it’s a field of four but it’s not nothing.
The podcast features Dr Blair Munford. Blair has been in the retrieval and prehospital field since the mid ’80s. He has stories. Lots of stories. This story is his though and in it you get to hear a little about what it’s like on the day you’re getting picked up by the helicopter. So maybe have a listen. Lots of people obviously thought it was worth it.
The Not Very Final Countdown
We’re not packing up or anything so it’s nothing like a final countdown, but is there a theme amongst the posts that people seem to click on the most? Well let’s see. Here are the 10 top written posts through 2017:
9. Tactics for hostile places – Tactical Medicine still going strong
The series on tactical medicine dates from 2016 but still gets plenty of interest. The third instalment just keeps clocking up the hits (and provides an easy link to chapters 1 and 2). People just want to know about phases of care I guess. If you like that you might also find this conference update worth your time too.
8. An old classic – little kid RSI
A couple in the year’s top 10 were all about kids which is a pretty pleasing thing. The care of kids isn’t just about shrinking stuff from adults and there’s plenty to gain from being kid friendly. This post went over the reasons that the approach to RSI in kids has changed and what we should be trying to focus on.
7. Necessity and the mother of invention
As much as we like kits sometimes you have to be flexible. This post on how to use what you have when you just have no choice is designed for when you’re stuck in one of those moments that will make you thank your gods for your real equipment when you’re back on a real job. Tourniquets? Check. Pelvic binding? Check.
This practical post on putting cannulas in little people certainly grabbed some interest. Maybe it will help out next time you’re facing a procedure that can cause pain at both ends of the needle.
3. More physiology when you pick a person up
This post comes from 2016 as well but it just keeps people coming up. A topic not covered that much elsewhere, but the physiology of a patient being winched is certainly relevant to lots of people in the rescue space.
We’ll level with you the rescuee here is apparently a mannequin so the physiology would be pretty forgiving but you get the idea.
2. In a bind
What is it about pelvic binders that gets people coming back for more. Our long running series on pelvic binders got a boost with number 5 which covered a case where the binder really probably didn’t help. You could drop by and end up down the rabbit hole of the other 4 posts with those links at the start of it.
1. Back to basics
And the top spot for 2017 goes to one of those great posts that covers things we often think of as basic but which might just make the biggest difference to patients – “basic” airways and adjuncts. Maybe you’d like to drop by this edition of those things we wish we’d known way back when we started.
So that’s the list. And the theme is pretty clear. People like practical things. And physiology. And things about kids. And things that touch on the literature. And … actually people probably just like all things prehospital and retrieval. Better get back to it.
Notes:
The image from unsplash.com was posted just like this by Neil Thomas.
There are a bunch of ways to figure out where to put your resources. Dr Alan Garner found a guy who can crunch the big numbers to look at it a little differently.
What’s the answer for optimal locations? First ask what is the question.
First up is a big thank you to my co-author Pieter van den Berg from the Rotterdam School of Management in the Netherlands. Pieter is the real brain behind the study and the mathematician behind the advanced modelling techniques we utilised. Pieter has looked at HEMS base location optimisation previously in Norway and has done some modelling for Russel McDonald’s service Ornge in Ontario, Canada as well. Without him the study would not have been possible.
So what did we do and why?
As already noted Pieter had recently done a similar exercise in Norway where the government has a requirement that 90% of the population should be accessible by physician staffed ambulances within 45mins. Pieter and his co-authors were able to demonstrate that the network of 12 HEMS bases easily accomplishes this – indeed it could be done with just four optimally positioned bases. They also modelled adding and moving bases to determine if the coverage percentage could be optimised with some small adjustments.
As it happens New South Wales (NSW) and Norway have very similar population densities and both are developed, first world jurisdictions. Hence this previous study seemed a good place to start for a similar exercise in NSW. Both jurisdictions also have geographical challenges; Norway is long and thin with population concentrated at the southern end whereas NSW has almost all the population of the state along the eastern coastal fringe with high concentration along the Newcastle – Sydney – Wollongong axis.
We were interested in population coverage but we also wanted to look at response times as this also is a key performance indicator for EMS systems. It is certainly reported as a key indicator by NSW Ambulance. Response times were not modelled in the Norwegian system so we were interested in seeing how the optimum base locations varied depending on the question that was asked, particularly in a jurisdiction such as NSW where the population is so concentrated to a non-central part of the state.
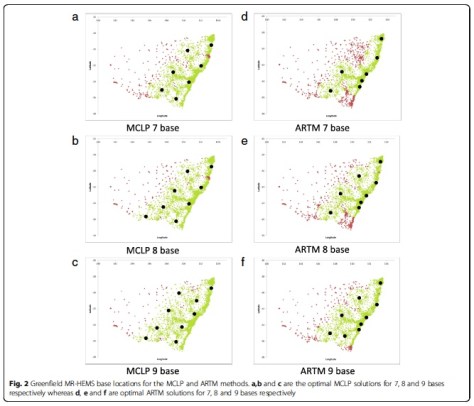
If you look at the study you will note from Figure 1 the existing arrangements in NSW. You’ll be shocked to know these arrangements weren’t planned in advance with the aid of a Dutch maths guru. These things happen organically. Nevertheless it provides a reasonable balance of response times and coverage although the gap on the north coast is immediately evident.
If you start with a clean slate and optimally position bases for either population coverage or average response time, both models place bases to cover that part of the coast (see Figure 2). Hardly surprising. When we modelled to optimise the existing base structure by adding or moving one or two bases, the mid north coast was either first or second location chosen by either model too.
This seems an obvious outcome from even a glance at the population distribution and current coverage in Figure 1. What is surprising is that the 2012 review of the HEMS system in NSW (not publically released) which utilised the same census data in demand modelling did not come to the same conclusion when two previous reviews in the 1990s and 2000s had recommended just such a change. Certainly the Reform plan for helicopter services which was released the following year did not make any changes or additions to base locations leaving this significant gap still uncovered.
Wagga Wagga was the other location identified for a HEMS base in the 2004 review. Interestingly it is favoured as the first relocated base when the existing structure is optimised for average response time by moving Canberra to this location. But a Wagga Wagga base also was not mentioned in the reform plan.
What about the green fields?
When the green field modelling was done it is clear that the current NSW system mostly closely resembles the model optimised for average response time, rather than coverage. The Wollongong base really justifies its location on this basis as it contributes to a better overall average response time. Its population coverage falls entirely within the overlapping circles of the Sydney and Canberra bases so it makes no contribution here, at least if a 45min response time is used as the standard.
There was another aspect that interested us compared with Norway. In Norway all aircraft have the same capability and this is also true for the recently tendered services in NSW. The unusual feature in NSW though (unique to Australia although common in Europe in particular) is a dedicated urban prehospital service operating from a base near to the demographic centre of the largest population density – Sydney. The performance characteristics of this service have been well described (by us, because I’m talking about the CareFlight service which I think does serve a useful function) previously and when it was operating with its own dispatch system was the fastest service of its kind in the world to our knowledge.
Like the Wollongong service it operates entirely within the population coverage circles of other bases, but it makes an enormous contribution to average response time. When this rapid response urban service is added to the network of large multirole helicopters in NSW the average response time across the entire state falls by more than 3.5mins because that service is able to access more than 70% of the state population within its catchment zone, and significantly faster than the multirole machines.
This modelling only takes into account the response time benefit of the specialisation afforded by such as service. We have previously been able to demonstrate that the service is also much faster in almost every other aspect of care delivering patients to the major trauma services in Sydney only a few minutes slower than the road paramedic system but with much higher rates of intervention and ultimately passage through the ED to CT scan faster than either the road paramedic or multirole retrieval systems in NSW. At least this was the case when it had its own specialised dispatch system but that is a story we have discussed previously too.
There are recurrent themes here. The Rapid Response Helicopter service adds significantly to the response capability in NSW whether you model it using advanced mathematical techniques or whether look at the actual response data compared with the alternative models of care. Indeed the real data is much stronger than the modelling. It seems that at least in large population centres in Australia there is a role for European style HEMS in parallel with the more traditional multirole Australian HEMS models that service the great distances of rural and remote Australia. Different options can work alongside one another to strengthen the whole system and better deliver stuff that is good for patients – timely responses when they really need them. The capability differences however need to be reflected in dispatch systems that maximise the benefits which come with specialisation rather than a one size fits all tasking model that takes no account of those significant differences.
Every version of the numbers I look at tell the same story.
Notes and References:
While this post covers a few ways of looking at a tricky sort of problem, there are lots of clever people out there with insights into how these things work. If you have ideas or examples from your own area, drop into the comments and help people learn.
Now, the paper that’s just been published is this one:
Well this time around we welcome a new contributor. Dr Shane Trevithick is a retrieval doctor with many years experience covering prehospital, interhospital and coordination work when he’s not being an emergency doctor. He’s got a bit on simple systematic approaches that get the job done.
One of the exciting things that practicing medicine out of a helicopter does is make you a “Rock Star” of the medical world. Your colleagues and the general public are amazed by your method of arrival on scene, the ensuing dramatic interventions, the sexy uniform, your appearance on the evening news and your general confidence back in the hospital when you can manage dramatic medical problems which seem much easier when they are not trapped upside down in wreckage.
The problem with being a Rock Star performing in a band is that to continue being the Rolling Stones of Medicine [Ed: we would not suggest this reference is in any way a sign of author age] you feel compelled to keep releasing new albums regularly. This can be a problem, especially with social media, as developments in medicine do not keep pace with the need to tweet and podcast and you are at risk of grabbing the latest study or technique involving patient plumbing and announcing this to the world as the next big thing in the world of Helicopter Rock Band Medicine.
This does tend to mean that you can gloss over some of the basic things which really make a difference to your medicine and your patients. Just like a Rock Star will be completely familiar with the basic things that makes playing their instrument possible, it helps if you can really nail the basics.
So here are a few tips that work for me to do a better job as a retrievalist in whichever team I’m working in. Have a Plan
A good plan when you approach a patient makes a big difference, especially for an interhospital retrieval. This makes a huge difference to the smoothness of how your retrieval will flow and reduces your risk of making an error by omitting something. This is a bit like having a checklist but I don’t quite use it like that because really a checklist involves a bit of call and response. It’s not quite a strict list, more like having a systematic approach to reduce the risk of error. If you have the same pattern to how you do things you get much quicker and slicker and you are much less likely to miss something.
It took me a lot of years to work out I didn’t have a consistent system. And when I analysed some the mistakes and complications I had I realised they came about because, like a good anaesthetic registrar would, I modified what I did to fit the Paramedic I was working with, rather than communicating a system that would ensure I didn’t miss things. If I had actually had any system to do the job myself then I would have avoided a lot of problems.
So here’s the system I created for myself. It might work for you, or might just prompt you to think through what system would work best for your brain.
A: Airway
Check ETT Size and measurement at a fixed point (e.g. teeth).
Check ETT Security – that means connections and how well it is tied/taped. I almost always find myself fixing something about security.
Check ETT Site – on an X-ray.
B: Breathing
How well is the patient breathing? It’s a seemingly simple step but yes, I still remind myself.
What are the ventilator settings? Got it, now match them (with the transport ventilator). I tend to work with paramedics who make logistics and practicalities in a brilliant fashion. It always seems that just as I get this step done they are ready with a patient slide to transfer the patient onto the stretcher.
C: Circulation
What’s the IV access? Secure that well too.
What about the arterial line? Critically ill patients being moved should have this so now is the moment to make sure it’s connected, working and zeroed. This usually matches up with when my friendly paramedic is miraculously also up to the exact bit where I should be helping with the monitoring.
D: Drugs
Think “I need enough sedation for 3 times the anticipated length of transfer” and make sure you’re ready (plus see the bit below).
Also have a think about what things you have handy as downers (mostly sedation and analgesia) and uppers (like metaraminol) which might just come in handy if you get the downers bit not quite right (or for other reasons of course).
E: Everything Else
Do you have all the equipment you brought with you?
Do you have the notes?
Do you have any scans?
Do you have ALL the equipment you brought with you?
Do you have any patient belongings, either the material ones or the relatives that also belong to them that you might be bringing?
No, really, do you have ALL the equipment?
Now, about that sedation
Yes, I gave this its own bit because it is really important. Let’s assume you’re highly skilled at drug-assisted intubation. After that there is the post intubation phase, whether you have intubated the patient yourself or whether the patient comes already intubated.
I think it is really important to make a couple of distinctions in retrieval. One is you are giving “a Retrieval” and NOT “an Anaesthetic” or “a Sedation”. An Anaesthetic is an art form so important there is an entire medical specialty devoted to it. But it is basically focussed on having someone pain free, unconscious of what item number is being performed on them, and then woken to a state of bliss in a a calm quiet environment surrounded by nurses fussing over you. Usually woken relatively quickly after the item number as well.
This does not apply to retrieval. In a retrieval you do not want your patient to wake up. Especially over that last speed hump on the roads leading to the hospital. With apologies to ICU that your retrieval patient will take a day longer to wake up than someone they lightly sedated you have to remember it is not a “sedation” it is a “retrieval”.
There is very little fussing (doctor dependant) and a lot of shaking up/moving/noise/vibration/stimulation. When I was a retrieval registrar no one discussed this with me and since I was very comfortable to treat people with morphine and midazolam either together or separately, with propofol, (ketamine hadn’t come into use again when I was a registrar) and with fentanyl I just kept running whatever the hospital had chosen assuming that since they were a hospital they had correctly chosen the right sedation for the right patient. It was also quicker and easier to just keep running whatever they started as we didn’t have to go through the entire fuss of drawing up new drugs.
I am now, with experience, absolutely sure that this is not best practice. Now I don’t use propofol at all for a retrieval – it is an ideal anaesthetic drug which makes it very poor for A Retrieval. Of course that is only my opinion born of experience with no published data I am aware of (there is a study for someone) however I can promise you that performing a “retrieval” after intubation requires only two drugs for maximum benefit: Separate infusions of fentanyl and midazolam. If you are running two inotropes and only have one pump left I will allow you to mix them together but the ideal concentrations are 1000mcg fentanyl in 50mL and 50mg of midazolam in 50mL. Run them at 10x higher doses than you would use in ICU so you need to think about starting at 200-400mcg/hr fentanyl and heading north and 5-10mg/hr of midazolam.
And if you arrive and your patient is light and coughing on the tube, if their haemodynamics will tolerate it just give them substantial loading doses of these drugs, say 0.1mg/kg midaz and 2mcg/kg fentanyl and then start your high dose infusion. I can promise you this will be the best tolerated, most cardiostable way of performing “A Retrieval”.
Just remember the gotcha – as your helicopter starts to land at the hospital it will shake violently for 30 seconds or so. This will cause your patient to wake up and extubate themselves at the one time you can’t go out of your seatbelt to fix the problem. Remember to bolus before landing.
So there you go. Some of the basics that can help you be the Rock Star you want to be.
Notes:
All the images here are via Creative Commons on flickr and are unchanged here and put up by Izzy by the Sea, Duncan C, ThoreauDown and Bart Everson.
If you have suggestions for future posts hit us up. And if you like the stuff around these parts, you could always consider sharing or signing up to receive emails.
Back with another instalment in the popular series “I wish I knew then what I know now” is Greg Brown, current Education Manager / Clinical Nurse Consultant with CareFlight and former Australian Army officer.
Intravenous cannulation: the art of finding the biggest tube with a sharp point in your kit and placing it in the most proximal vein you can find so you can deliver various fluids or medications that may or may not make the patient feel better but certainly help you feel as though you have achieved something.
Okay, this might be a bit of a stretch – but in all seriousness the ability to gain and maintain dedicated vascular access in your sick patient is a vital component of medical care for nurses, paramedics and doctors alike. For many (both in and out of hospitals), the ability to find that elusive vein is a point of pride, and getting that solid red flashback in the chamber of the cannula is at times the cue for the treating team to stop holding their breath.
But the IV cannulation process is not complete once the [insert name of your service’s approved form of IV dressing] is applied. In the retrieval world, an IV cannula is almost always going to have fluids flowing through it (or at least attached to it). Having fluids attached gives the healthcare provider a ready-made flush for those medications that are used in treating the patient. Want to give a bolus of IV ketamine? You are going to need an IV flush. IV fentanyl? Flush. IV anything? Flush. You are going to be flushing everything, so you might as well attach a 1000mL bag of “flush” via a giving set and have it ready at all times.
Herein lies the problem. For anybody who has ever had to move a patient with an IV line attached, you know just how easy it is for that line to get snagged – and before you know it, your precious cannula is now no longer in a vein and instead is irrigating the helicopter floor / CT machine / footwell of the crashed car etc. Your service’s approved form of IV dressing might be awesome at holding an IV cannula in place, but it is no match for the body weight of that burly rescue technician with the IV line inadvertently wrapped around his leg who is moving in the opposite direction to the patient.
Laws to Live By
Many years ago at CareFlight, one of our “grey beards” (Dr Blair Munford, anaesthetist extraordinaire), came up with what we now call ‘Munford’s Law of Taping’ which states:
“The length of tape used on the patient should not exceed the distance between the point of injury and the receiving hospital, but anything less is acceptable.”
Taping IV lines is a good thing, but tape doesn’t work great on wet, hairy or dusty patients. Sure, you can circumferentially tape the IV line to the arm such that the tape sticks to itself and not the patient, but that is a lot of non-stretchy tape.
Story time. Many years ago, whilst on deployment with the Army, I was tasked with transferring a civilian casualty from the scene of a vehicle accident to a landing point whereupon she was to be whisked away to a United Nations hospital by helicopter. The accident involved an overcrowded minivan which failed to negotiate a corner resulting in it rolling. The knock-on effect was a mass casualty incident halfway between two forward operating bases. Medical and security assets were despatched to the scene, including myself as a young (ish) nursing officer.
After the usual initial chaos that results when medicine and tactics collide, we dutifully set about the triage and treatment of casualties in accordance with priorities and started stacking inbound AME assets. Unfortunately, given the topography, the AME teams could not land on site; therefore, we were required to ferry the casualties from the scene to a landing point about 2km away.
One particular casualty of mine was a lady with a mid-shaft femur fracture and a handful of broken ribs. I had applied a Donway Traction Splint to the leg, some oxygen and was trying to bump up her blood pressure with crystalloids whilst controlling her pain with increments of IV morphine. I had placed an IV in her antecubital fossa and had “secured” the giving set with some tape. However, despite the accumulative administration of a lot of morphine (the exact dose escapes my memory), she was still very obviously in pain. The problem? As we loaded her into the vehicle, the IV line became looped around the stretcher handle and the cannula had dislodged.
Ordinarily I’d have just placed another IV and started again; but in this case I had two problems: (1) being a mass casualty incident my stores had been pillaged leaving me unable to place another IV, and (2) the Blackhawk was already flaring (meaning it was about to land), so I didn’t have time to go back to the scene to grab more stuff. This was a major fail when it came to managing this patient. And in addition, the woman’s pain and lack of analgesia were about to become the AME team’s problem, but the embarrassment of losing the ONLY IV access this patient possessed was mine alone.
But, in the words of S.E. Hinton, “that was then, this is now”.
Simple Solutions
There exists a remarkably simple solution to this problem, and it involves a bandage. We now teach this technique to anybody who will listen because, quite simply, there is no good reason for losing an IV. It works on the side of the road; it works in an ambulance; it works in Emergency Departments; and interestingly, it works really well in those dementia patients that occupy their time by trying to undo every single medical intervention you’ve applied during your 12 hour night duty!
Step 1: Place an IV cannula in your patient in accordance the patient’s need and your ability / scope of practice. Apply whatever dressing your service says you should.
Step 2: Attach your primed IV line as per the application of common sense. Ensure that the roller clamp on the line is as close to the bag as possible – you will need to be able to access it.
Step 3: Run the IV line down the limb around 10cm / 4in and cover in a bandage (the broader the bandage, the faster the technique), leave a loop then bandage the IV line back up the limb.
Step 4: Repeat step 3 ending with the free running end of the IV line heading towards the head of the patient (this is where you will be located; if you need to replace the IV bag it’s best if the bag is close to you).
Step 5: Secure the end of the bandage with some tape. Ensure that you leave the side injection ports of the IV line accessible. You may even wish to mark these with tape so that you can find them quickly when under stress.
When you secure the IV line with these superimposed S bends you create 40cm of dead space that will take up the strain on the line if the line is pulled. Once tension is applied to the line the loops cinch together to take up the strain. More of a visual learner? Yeah, me too. See the images below.
What I now know that I wish I knew then is that performing this technique takes no longer than trying to apply copious lengths of tape to a patient’s arm, especially when that arm belongs to a sweaty, hairy person. I also know that I never again want to be the clinician whose handover includes “well, there was an IV in the arm but I kinda lost it in transit…” If it is worth doing, it’s worth securing.
Notes:
We bet this isn’t the only way to secure a line. Got tips for us to learn? Then put them in the comments. We like learning.
And remember if you like stuff on here, have a think about sharing it around. And maybe sign up to get an email when a post hits.
Contributors Dr Toby Shipway and Flight Nurse Jodie Martin return with a little about something that would make any retrievalist sweat – delivering babies in the air.
A call came into the Logistics Coordination centre from a nurse in a remote health centre, worried about new contractions in a pregnant woman who was 31 weeks pregnant. We decided to take a full retrieval team for the ‘just in case’ scenario. Afraid of getting caught out, we had a big discussion to make sure we had all the right gear on board the aircraft and what our plan of action would be should we be faced with the rare event of an inflight birth. Why worry though? They’re rare, right?
We retrieved the woman from a remote airstrip and it became evident just after takeoff that she was in established labour. Even after tocolytic therapy, the preterm baby was born at the start of descent into Darwin. No one on the plane will forget the midwife examining the patient, looking up wide-eyed and shouting calmly down the plane ‘its coming out now’. Never has a pilot descended at such a pace. After initial resuscitation of the baby, both mum and baby did well and were transferred safely to the hospital. Phew.
After this, we started researching how many in-flight births had been registered during CareFlight’s tenure in the Northern Territory (NT). This became the basis for a recent case series publication in the Airmedical Journal.
The sort of view you don’t get to enjoy when it starts getting imminent.
The Big and Little Numbers
Four cases were found on searching through the database over a four-year period from 2011 to 2015. Over that four-year period there were 1311 retrievals associated with Obstetrics and Gynecology, out of a total number of 15967 retrievals in the NT. This means obstetric and gynecology related retrievals account for approximately 8.2% in our aeromedical retrieval service.
Looking at the obstetric retrievals in more detail, there were 436 cases associated with pre-term labour of which 4 progressed to in-flight births. This equates to an incidence of 0.92% of all women transferred in preterm labour. It is not a common clinical situation.
Here’s a brief description of each of those 4 cases.
Case one was a 37 year old woman of gestational age 36+5 weeks, gravida 5 para 2. The retrieval was tasked in the early hours at 0010. Take off was at 0050 and contact was made with the patient at 0145 at the airstrip. She was contracting 3:10 at this point. Tocolytics had been administered according to protocol, which was 3 separate doses of nifedipine 20 mg initially, at 30 mins and at 1 hour. Return takeoff was at 0210 with progression to spontaneous vaginal delivery of the baby at 0245. 10 unit of syntocinon was administered intramuscularly with approximately 300 mL of blood loss measured with delivery of the placenta. Apgars of 61 and 95 were recorded. Both baby and mother were discharged at 3 days from hospital with routine follow-up from the community nurse.
Case two was a 25 year old woman of 31week’s gestation, G2P1 – this was the case from the top. Again this was an early morning flight, tasking was at 0052 and take off was 0128. Patient contact was made at 0250, where the patient walked onto the plane contracting 1:10. The clinic team had given nifedipine as per protocol. Return takeoff was at 0300 with progression to spontaneous vaginal delivery at 0400. Apgars were 61 and 85 with the baby needing some supportive ventilation. Mother and baby were transferred to hospital where on assessment in the neonatal unit positive pressure ventilation was stopped. Length of stay for this little one with intrauterine growth retardation was 22 days; there were no complications with the mother.
Case three was a 31 year old woman of 22 week’s gestation, G6P2. This one came up in a previous post as it involved a complicated resuscitation of mother and baby. The midwife was en-route back to home base on another task when the referral call to divert to this case was made. This again was in the early morning with the re-tasking occurring at 0330. On assessment at 0450 the patient was contracting 3:10, and the clinic reported a large clot was passed in clinic. Return takeoff was at 0500, with progression to spontaneous vaginal delivery at 0522. Apgars were recorded as 61 55 510 as neonatal resuscitation was ongoing. The mother delivered the placenta at 0548, which was accompanied by a PPH of 1 L dropping maternal BP to 42/38. Fundal massage and a blood transfusion were started. On landing the retrieval team was met by a ground crew – the neonate was transferred in a separate ambulance with ongoing resuscitation by the Medical Retrieval Consultant and a flight nurse. On reaching the Emergency Department the multi-disciplinary team decided to cease resuscitation of the baby at 0645. The mother received further blood products and stayed in hospital for 4 days.
Case four was a 26 year old woman of 28+5 week’s gestation, G2P1. This was the only retrieval in daytime hours with tasking at 1040 and take off recorded as 1135. The retrieval team went into clinic on arrival, making contact at 1245. On assessment the patient was contracting 1:10. Return takeoff was at 1345 and patient passed a large blood clot at 1410 with rapid progress to spontaneous vaginal delivery at 1418. Apgars recorded were 61 95 and some respiratory support with nasal high-flow was given. The placenta was passed at 1425 and the total blood loss was estimated to be 250 mL. The patient had no documented cardiovascular instability. The patient and baby were transferred to hospital with no further issues. However the baby stayed in hospital for 66 days needing long-term respiratory and feeding support. It was diagnosed with a dilated cardiomyopathy and on follow-up review was listed for a heart transplant.
What About the Treatment?
All women received the recommended preterm labour treatment, being intravenous antibiotics and steroid therapy. Three out of four patients received tocolysis – the fourth case did not as the blood clot passed in clinic was deemed a contraindication. It was reported vaginal examinations upon referral were conducted in 3 out of 4 of these cases. Interestingly, the reports of those examinations found the cervix to be closed or an undetermined dilation. It goes to show that despite our best estimates from a physical examination we need to be prepared that inflight birth may in fact occur, even though it is a rare occurrence.
In transferring women in pre-term labour, the aim is to keep the baby in utero, as the evidence relevant to our setting indicates that in utero transfer is associated with much improved maternal and neonatal outcomes. The NT has a particularly high proportion (10.6%) of preterm births prior to hospital arrival and although multifactorial the large distances are likely to play a significant role. Prompt retrieval and the involvement of a team with the right skill mix to make a detailed obstetric/midwifery risk assessment would hopefully lessen the chances of inflight birth. But very rare still doesn’t mean never.
Last time Jodie Martin, Flight Nurse extraordinaire dropped by she shared one of our most popular posts ever. Jodie returns with a little on the Top End experience of sepsis.
Time for a look at some remote medicine again.
CareFlight provides the aeromedical service for the top half of the Northern Territory (NT) in Australia. The area covered by the service is the same size as France but has only 160,000 people. And less vineyards.
As 115,000 of this population are in Darwin which is serviced by road ambulance services this leaves CareFlight to provide services to about 45,000 people in very remote and widely scattered centres, most of which are small Indigenous communities. The catchment area has only two rural hospitals which are non-referral centres with care otherwise provided in remote health clinics. Even then not everyone lives close to a rural hospital or remote health clinic. Some rural folk still have to drive several hours or even a few days to any level of health care. Access to health care is a real challenge when someone becomes sick.
The Top End of the Northern Territory may be sparsely populated with 0.2 persons per square km, but it has the highest incidence of sepsis in Australia and five times higher rates than those recorded in the US and Europe 1,2. It has been suggested that one of the reasons for the high incidence of sepsis is related to the higher Indigenous population in the Top End 2. The incidence of sepsis requiring ICU admission in the Top End of the NT for Indigenous people is reported to be 4.7 per 1,000. In the non-Indigenous population there are 1.3 admissions per 1000 people. When compared to the rest of Australia, the rate of admission to an ICU for sepsis is 0.77 per 1,000 2 with national 28 day mortality rates of 32.4% 1.
The Top End – Not Just Popular with People
Human-invading bacteria and viruses love the warmth and moisture of the tropics. To make things even harder, the Top End has the highest rate in the world of melioidosis, a very nasty pathogen found in the wet tropics of Australia. Melioidosis has been classified as a Type B bioterrorism agent by the Centre for Disease Control in the US and kills up to 40% of infected patients often from rapidly fulminant disease. However most sepsis is of the more common garden variety, but still causes severe, life threatening illness.
A quick editorial note that we have done another story from the Top End and still it’s not about crocodiles. We apologise but it turns out there are other things up there trying to kill you.
When you add the challenges of distance and retrieval times, meeting targets for sepsis treatment which are time-based would seem an impossible task. Given this, we were keen to review the retrieval of septic shock patients in our service to see what the outcomes are like and whether we could improve the process. The results have just been published in the Air Medical Journal which you can find here.
The patients were sick. A third of patients required intubation and 89% required inotropes. Median mission time however was 6 hours and the longest case took 12 hours. Given the remoteness and time delays inherent in retrieval over such distances with a population known to have worse health outcomes, you would expect mortality to be high. Surprisingly however the 30 day mortality in this group of 69 patients, which are predominately Indigenous, was only 13%. This is lower than previous rates described for both sepsis in Australian Indigenous populations and for patients in Australian and New Zealand intensive care units.
That’s Excellent, But Why?
It is interesting to speculate on the possible reasons for such good outcomes. Reasons might include:
The relatively young age of the patients compared with many series. Perhaps the better physiological reserves of younger patients are still a key factor despite the higher rates of co-morbidities.
Early antibiotics – these are almost always given by the end of the referral call. Good clinical coordination has a role to play in this too.
Early aggressive fluid resuscitation – the median volume of crystalloid administered was 3L during the retrieval process.
Inotropes administered following fluid resuscitation occurred in the vast majority of patients.
Early referral – recognising when a patient is sick. This is something we’d like to gather more data on. We didn’t record how long a patient was in a remote health centre before a referral call was made, but we have a suspicion early referral might have played a part here.
It is also interesting to note the good outcomes that were achieved without invasive monitoring in approximately half the patients retrieved. Perhaps there are shades of the findings of the ARISE study here where fancy haemodynamic monitoring really did not seem to make much difference either – what matters in the retrieval context is early antibiotics, aggressive fluid resuscitation and early intubation when indicated.
We did not randomise patients to invasive versus non-invasive monitoring and it is possible that the sicker patients and those with longer transport times received the invasive version. But it is also possible that we get too hung up on this stuff and it is the basics that really matter whether you are in the city or a really remote health clinic.
The Wrap
The Australian Indigenous population have poorer health outcomes than the general community. Outcomes are even worse for those residing in remote areas than those in urban areas. In our small study it is pleasing to see such good outcomes despite remoteness and long retrieval times. Our young patient cohort recovered well considering how sick they were but what would be even better is preventing sepsis in the first instance. The incidence and burden of sepsis in young Indigenous people requires preventative strategies and appropriate and timely health care resources. Improving access to health care, improved housing and decreasing overcrowding, decreasing co-morbidities and decreasing rates of alcohol and tobacco use are hopefully just some of ways we can possibly decrease the incidence of sepsis and contribute to closing the gap.
Notes:
That croc with almost enough teeth came from flickr’s Creative Commons area and is unchanged from Jurgen Otto’s original post.
Here’s the link to the paper that’s just been published:
This post from Dr Alan Garner tackles a core problem for all practitioners who give a damn – how do you know you’re doing it well? A chat worth having and Alan has a pretty good summary of the Carebundle approach.
How do we measure quality in prehospital and retrieval medicine? Speed? Number of procedures performed? Number of twitter followers?
Seriously though, this is a question that vexed me for many years as a service director and trying to find metrics that measure things that mattered seemed an elusive task. The major part of the problem stemmed from the heterogeneity of the patient population that we treat. Even simple (but easily measured and therefore attractive to bean counters) things like timeliness are not straightforward. Not because they are hard to measure but because sometimes time matters and other times it very clearly does not. Indeed emphasising it as a measure could lead to perverse outcomes for some patients.
Let me give you a couple of examples to illustrate the problem:
Case 1. Central abdominal stab wound with hypotension.
There is almost no prehospital intervention that matters in this patient except gasoline and perhaps tranexamic acid. I don’t think anyone would argue that time is a reasonable quality measure in this patient.
Case 2. COPD patient in a small hospital an hour flying time from the nearest intensive care unit.
Patient is eventually stabilised on non-invasive ventilation after three hours of effort by the transport team at the referring site. They are then safely transported. Clearly for this patient time does not matter at all. Reporting turnaround time at the referring site in this patient may place subtle pressure on the team to intubate the patient early and depart – a move that is very clearly not in the patient’s best interests and would have placed the patient at significantly increased risk of unnecessary morbidity and mortality.
This got me thinking that our measures of quality had to be disease process specific or we were never going to move forward. Speaking with Erwin Stolpe was the turning point in my thinking.
You Should Really Try to Know Erwin
Many of you will not have heard of Erwin. Sometimes when I talk to people or read things on social media I get the impression that physician staffed HEMS started in about 2005. The reality of course is quite different. Erwin is a trauma surgeon from Munich who began flying as a resident on the Christoph 1 service out of that city in 1968 (yes, not a typo – 1968).
Here he is, at AirMed 2014 in Rome.
These days he no longer flies but is chair of the ADAC medical committee. For those unfamiliar with ADAC they run about 35 physician staffed HEMS bases in Germany and also operate several jets for longer range transports. Their HEMS services alone conduct about 50,000 prehospital cases annually. The breadth and depth of experience of this organisation is extraordinary and Erwin has been there from the beginning. You would think there might by a few pearls of wisdom there and you would be right.
The Key Cases
Erwin described to me the “tracer diagnosis” process they use to track the quality of the care that they provide. Analysis of their prehospital caseload indicated that four diagnoses made up 75% of the cases they attended. For these four diagnoses they defined the treatments that they expected the teams to achieve (see pages 52 onwards of this presentation by Erwin for more detail). They used national and international consensus guidelines as a base. They then began reporting against those criteria and they have also started to publish that performance.
What Erwin was calling “tracer diagnoses” is probably better known to us in the English speaking worlds as a “Carebundle”. Lots of people will be familiar with the ventilator Carebundle for intubated patients in the intensive care unit. Adherence to the items in the bundle is associated with lower rates of ventilator associated pneumonia. In NSW and Queensland, Health Departments have introduced bundles for central line insertion in order to tackle the rates of central line associated bacteraemia. In this case the bundle applies to a procedure or process rather than a diagnosis. Is there a place for this kind of methodology in the prehospital and retrieval world to improve quality too?
What are we talking about when it comes to PHARM?
Let’s start by looking at what a Carebundle is.
“A bundle is a structured way of improving the processes of care and patient outcomes: a small, straightforward set of evidence-based practices — generally three to five — that, when performed collectively and reliably, have been proven to improve patient outcomes.”
This definition is taken straight from the Institute for Healthcare Improvement (IHI) website. There is a bit of controversy regarding whether the items in a Carebundle really need to all be completed for the bundle to be effective in some sort of synergistic way or whether they are in fact just a checklist of items that have been shown to be effective and you get as many done as you can. I am not aware of any evidence for the synergistic effect multiplier that is implied on IHI website. I think it is unarguable however that you should try and get as many of the things that are proven to make a difference to that condition completed as possible. That is certainly the approach that we have taken.
Another quote from the IHI website describes for me what we are trying to achieve by using bundles:
“The power of a bundle comes from the body of science behind it and the method of execution: with complete consistency. It’s not that the changes in a bundle are new; they’re well established best practices, but they’re often not performed uniformly, making treatment unreliable, at times idiosyncratic. A bundle ties the changes together into a package of interventions that people know must be followed for every patient, every single time.”
Using Carebundles in hospitals is clearly not new. Even in EMS it has been previously described for benchmarking purposes. The attraction of the methodology for me was that we would know if our care for patients with severe head injury for example was following the best available evidence and we would know what proportion of our patients were receiving that care. I did not want just some of our patients to get that care, I wanted all of them to get every item of care that we could identify matters for that disease process all of the time.
Making it Match What We Do
For our rapid response service in Sydney we then determined from our medical database the diagnoses that cover 75% of our caseload as ADAC had done. For us this resulted in the following list:
Multiple blunt trauma
Isolated severe head injury (GCS<9)
Burns (>15% BSA)
Penetrating trauma
Immersion/drowning
Seizures (to which we were often being dispatched as they were mistaken for head injury or had caused a minor traumatic event)
ROSC post primary cardiac arrest (similar to seizures – trivial traumatic injury and patient in VF)
Traumatic cardiac arrest (for us this is the HOTTT Drill which I have described in a previous post, well podcast but which also includes the HOTTT Drill package to go with it).
We then turned to the evidence based consensus guidelines, Cochrane reviews and good quality RCTs to define the Carebundle items. This is a sobering process as you realise just how few interventions there are that have good evidence to back them up. This is particularly true for prehospital care where we are often operating in an evidence free zone. In many cases we had no choice but to go with the consensus (or best guess as I like to call it). We decided that we would include intubation for unconscious trauma patients for example despite the evidence not being all that strong and in many cases contradictory.
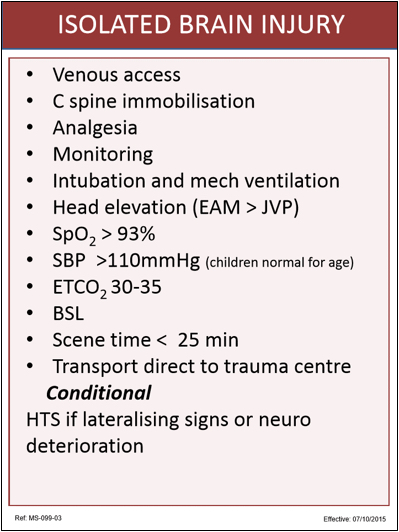
When we had defined the items for the specific diagnosis we printed them up on cards that team members carry in their pocket. These serve as a checklist which teams use on site or in transit just to be sure that they have covered all the items. Below is our isolated severe head injury card – the item I constantly forget is the blood glucose level (BSL). Highly embarrassing if this is low when you arrive at the trauma centre! I for one am glad to have the prompt.
Some of these items are extrapolated from in-hospital care. For example having the external auditory meatus (EAM) above the JVP makes sense in terms of managing raised ICP but there is no direct prehospital evidence that shows this changes outcome. We have also set relatively conservative targets for things like oximetry and blood pressure. Most of the evidence suggests SpO2 >90% is enough but we felt that desaturation happens very rapidly from this point so we would rather aim a little higher.
Aspirations and Signals
Some of the items we knew from the outset that we would never achieve in all cases. Scene time of <25mins is the obvious example. When a patient is trapped this is outside of our control. We know however that one in five patients with a severe head injury will have a drainable haematoma that is time critical. We therefore included this item in order to signal to the team that we expect them to treat severe head injury as a time critical disease in the prehospital phase.
Some of the bundles have conditional items as well. For head injury this is the hypertonic saline which we only expect to be given if there are lateralising signs or neurological deterioration.
When the team returns to base they complete an audit form indicating if the bundle items were achieved and if not, the reason for the variance. This both reinforces for our personnel the contents of the bundles and also allows us to report on compliance. Below is an example of our report for severe head injuries showing the reasons of variance in the comments section.
You can see that we don’t meet all the targets all the time, and there is usually a good reason when we don’t. However the Carebundles allow us to be transparent about what we think good care is, and also about how successful we are in achieving it. We include Carebundle compliance (along with a lot of other stuff) in our external reporting in NSW to the Ministry of Health, NSW Ambulance, The NSW Institute of Trauma and Injury Management and all the trauma centres to which we transport patients. Transparency is a key component of good governance and this processes helps us to achieve that.
Those People Were Here First
The concept is not new. I merely walk behind the giants of the industry and follow their lead in this. It is also worth noting that Russell MacDonald from Ornge in Ontario is leading a similar project with an initial group of 10 “tracer diagnoses” amongst a small international collaboration of critical care transport providers. It will be interesting to see how closely their bundle items accord with our own. Aligning our bundle items would allow us to benchmark ourselves against similar organisations in other parts of the world and create opportunities for us to learn from organisations who manage specific conditions better than we do. In the end this is about maximising the outcomes for our patients and I will gladly accept any help I can get in achieving that.
Notes:
Here’s the stuff referred to along the way, because the originals remain a vital part of looking at the issue.
It’s very pleasing to have a new contributor on this site. Toby Shipway is an anaesthetist with a special interest in prehospital and critical care medicine. He has worked on and off in the Top End of Australia with CareFlight undertaking all sorts of missions.
After researching the topic of in-flight births, I found out about one particular retrieval involving a midwife from work. On some downtime at the base she described a little about the case. A referral was communicated when she was already returning from a retrieval job with a patient onboard. She was to be re-tasked to a pre-term labouring mother of 22 weeks gestation an hour’s flight away from Darwin. An urgent transfer was requested because the patient was attending an isolated clinic with no midwife services or specialist paediatric facilities.
She was the only midwife available on shift but with a sick patient already on board. The mother gave birth just as the plane reached cruising altitude and the baby needed lengthy resuscitation with APGARs never exceeding 6. The mother, who had been given nifedipine for tocolyosis, delivered the placenta several minutes later and had a post partum haemorrhage of 800-1000mls, dropping her blood pressure to 45mmHg systolic.
You can feel a long way from anywhere in the air over the NT.
The nurse was suddenly balancing the needs of two critical patients, with no support. She managed to start an urgent blood transfusion, draw up appropriate drugs and set up oxygen for the mother, put monitoring on the baby, perform intermittent bag valve mask support, address it’s dropping temperature and maintain communication to a beleaguered pilot. After landing they were met by doctors, nurses and paramedics to get mum and baby to hospital. Unfortunately the premature baby did not survive, passing away 2 hours post delivery. The mum responded well to ongoing treatment and was discharged several days later.
The nurse looks back on the case with regret and a feeling that events should have occurred differently, although all who reviewed the case praised her efforts. She remembers waking up that evening, her arms cradled as if still holding the baby. How do we move on from challenging cases? How do we deal with the emotional footprint left behind?
The Stuff They Forgot To Teach Us
The emotional impact of medicine on clinicians is a topic rarely addressed throughout medical careers. Medical and Nursing Schools devote little or no scheduled time to the topic with so much content vying for timetable space. However, as we step onto the wards it takes little time for complex patient situations, tricky professional relationships, or the erosion of personal lives to ambush the newly qualified. The difficult choices made by medical professionals and their profound effects on patients can cause considerable anxiety and self-doubt. We are, on the whole, naïve and under-prepared for these situations.
Pre-hospital medicine is a unique environment for patient care. The intimacies of one-on-one care, the patient’s fearful confrontation with their illness and the alien experience of the plane or helicopter emphasise a feeling of vulnerability. From a medical perspective, it is a contained environment, which means minimal external sources for advice and an enhanced feeling of personal responsibility.
The empathetic manner of clinicians is rightfully promoted as an integral part in the care of patients. ‘Bedside manner’ and ‘empathy’ became buzzwords in medical education with the aim to instill the patient’s perspective into the clinician. The ability to empathise with patients builds trust, empowers patient’s decision-making and leans away from clinical paternalism. Empathy also brings us emotionally closer to patients. The pain and suffering witnessed by medical professionals is an aspect of the job to which we become accustomed but exerts a significant emotional toll. This can play out in all manner of ways depending on the individual involved.
We do know more about this than we used to. Although rates of depression have not been found to be higher than the general population, rates of anxiety, substance abuse (in particular abuse of prescribed drugs), and suicide are higher than the general population. In particular female medical practitioners were found to have a 146% higher risk of suicide, with males at a 26% higher risk compared with the general population. Several barriers to seeking help have been identified including concerns about stigma, career development, impact on patients, confidentiality, embarrassment and professional integrity.
However, humans have an amazing capacity to adapt and the efforts of supportive colleagues, a non-blaming environment and the breaking down of the clinicians ‘unshakeable’ image are part of the solution to a complex issue.
The midwife recalls the case with sadness but from informal discussions at work and review of clinical notes it became evident that her handling of the case was outstanding. It really was the worst case scenario with a mixture of two critically unwell patients, a difficult environment, limited resources and a long time in isolation before clinical help could be sought. It was a credit to her and the people supporting her that she was back flying so quickly after.
Notes:
Those stats come from this report released by Beyond Blue:
It is very exciting to introduce Tim Wallace, flight nurse from the Top End, on a topic sorely neglected for a website coming from Australia – animals that can kill you. Actually, perhaps Tim can introduce Tim.
“When I was a researcher working for a haematologist, I wanted to be a paramedic, but I ended up as a pedantic number chaser driving ventilators (ICU nurse). So I went to uni again so I could be a paramedic. Then I got this job and now I’m studying midwifery (I’ve been a uni student for 9 of the last 15 years). I came to Darwin then left after a couple of years and went rock climbing for a year with my now wifey. I thought the grass was greener down south. It wasn’t. I like Darwin. Finally, I think cats are the only malicious animal.
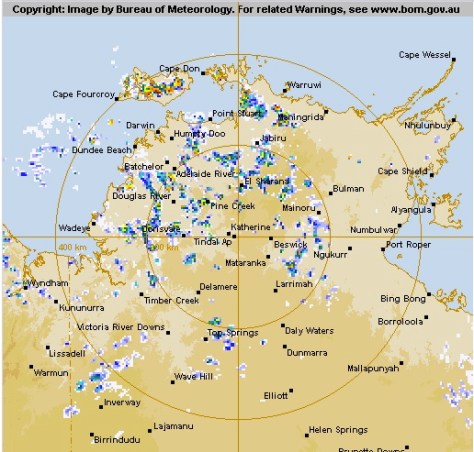
It’s 11 p.m. one night, in the middle of the wet season and a referral comes in for a suspected snake bite in Bulman. What? You don’t remember where Bulman is? Perhaps refresh your geography here.
Here’s the stuff you find out straight away:
A 34 year old male has been bitten by something on the foot.
He presented around 1 hour before the phone call with a story of walking along the road and stepping on a snake that then bit him. Bearing in mind that an Indigenous man from a very remote area like this is probably very familiar with the characteristics and behaviours of the local wildlife, this man says he didn’t see the snake, but felt it and has some marks on his left ankle that could be puncture marks.
He walked to the clinic (1km) and since then has had the leg immobilised and a pressure bandage applied.
His observations are unexciting and he is completely asymptomatic of any of the obvious signs (e.g. bleeding from cannula sites) or often subtle symptoms (e.g. abdominal pain) that might be associated with a snakebite.
So what do you make of a story like this? Well typically in a case like this a lot of emphasis is placed on the story as there are a lot of variables (and ambiguity) associated with confirming a snake bite and predicting the clinical course, including:
What first aid has actually happened? Was it immediate or delayed, effective or ineffective?
Timing: while a bite from a brown snake can be almost immediately obvious, death adder neurotoxicity may be delayed as long as 24hours.
Syndromes of envenomation have very poor specificity in general (see ‘syndromes of envenomation’ table/picture)
You often see dry bites where the snake digs in with the fangs but does not inject venom.
Then there are stick bites, such as: did not see snake, but felt something while walking in the bush at night.
Let’s Talk Logistics
Back to our patient – how will we get there?
Bulman is ~550km as the Kingair flies and is exceptionally isolated and now has no emergency medical services (as they are all tied up with this case). The strip is unlit and not suitable for night landings. While it is possible to get in using the helicopter, there is a large band of storms between us and Bulman that means a bumpy marathon of a flight in what one of my colleagues calls the ‘vomitron’, stopping for fuel via a detour to the north of Kakadu on the way there and back.
Yeah. It’s not going to be easy.
Are the Snakes Dangerous?
Well everything in Australia is designed to kill you and the Top End is the most Australian bit of Australia. We have some awesome elapids (hollow fixed venom injecting fanged snakes) up here and snakebite is an increasingly common emergency presentation (as you will see from our data). Australia sees ~3 fatal snakebites per year + occasional significant morbidity (e.g. mechanical ventilation, neurological sequelae at discharge).
Most of the mortality is associated with the brown snake family whose victims classically present with a story of early collapse and go on to develop VICC (venom induced consumptive coagulopathy) and occasionally signs and symptoms of neurotoxicity. In the Top End, in addition to the western brown, the other problematic species are the myotoxic king browns (mulga snake), neurotoxic death adders and less commonly the mighty taipan (VICC, neurotoxicity). Many of our retrieval registrars come from countries with boring fauna and this topic is very exciting for them.
Not very specific really. (This table is from the Isbister paper mentioned below.)Fun fact: the bite reflex of some snakes can remain intact for over an hour after death. This is me playing with a dead brown snake brought in by CareFlight (with a patient) before I was familiar with the case reports of envenomation from dead snakes …
Having posed this scenario to a few of the retrieval consultants at CareFlight they all placed significant emphasis on how convincing the story was and all offered varying perspectives on the priority of retrieving this man. Remote clinics use the ‘CARPA Standard Treatment Manual’ protocols for managing emergency presentations, and CARPA is quite clear about snakebite:
And we can’t assume the RAN was comfortable by herself with this guy in her clinic.
It turns out that the capacity to deal with a sick person might be more limited than the hospital …
Despite the rigid proclamations of the CARPA manual, I reckon there are unanswered questions about when (and if) patients who are suspected to have been bitten by a snake should be retrieved. As I have alluded to, confirming a diagnosis over the phone is difficult and a lot hinges on how convincing the story is. With this in mind we decided to try and arm ourselves with some hard facts, undertaking an audit of our retrieval database to quantify the existing situation around suspected snakebite retrievals.
Maybe there’s another time to take the ex-snakes back to the city? (And the patients, of course.)
Let’s Talk Numbers
Interestingly, the numbers of retrievals have increased somewhat since the last published data:
– Currie (2004) – 8.6 year sample – 13.6 aeromedical retrievals per year
– Our audit – 3.8 year sample – 30.2 aeromedical retrievals per year
Why? We’re just not sure.
When it comes to confirmed envenomation we get to a very select group:
– 3.5% (4 of 115 patients) – we’ve used antivenom twice in this period
The comparison? Well previously published data for northern Australia has quoted 5-23%.
Why are those numbers for confirmed envenomation lower in our stats? We don’t quite know that either.
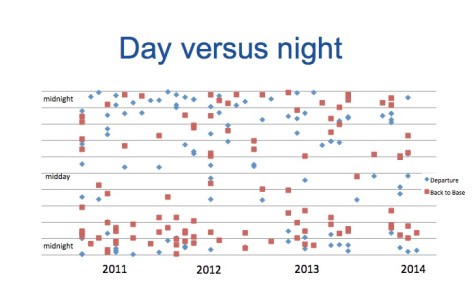
Then there’s the when – is there any particular time of day when the calls come in? Well ~65% of retrievals occur at night – see the slightly busy plot of night retrieval timings
Of course, the timing also has some implications for our pilots.
Flying High
In the Top End strips vary from well serviced, long, sealed, well lit and fenced in with GPS approaches (eg. Gove, Groote Eyeland) to poorly lit, narrow, occasionally dirt strips that are actually primarily the homes of kangaroos and buffalo and only occasionally used to land aircraft. The lights in many remote strips are solar, so they are great at 11pm but generally a lot less bright by 3am.
Crucially, many of these strips have no GPS approach. Where there is a GPS approach, the avionics aid the pilot in landing. Where there is no GPS approach, the pilots do a ‘visual circling approach’. What does that mean for safety? Well night flying is 3 times more dangerous than the equivalent aviation work in daylight hours. A visual circling approach is 25 times (!) more dangerous than a GPS approach. 25 times. (As a sidenote, helicopter EMS operations are also more dangerous at night.)
Perhaps the best insight for the aviation lay-person is to watch this video of a visual night time landing filmed by one of my colleagues on an after hours retrieval.
How were you planning to get there again?
Back to the Bitten
Back to our dude in Bulman. The retrieval consultant, in consultation with the logistics coordinator and flight crew decided that the the face of apparent low risk to the patient and massive logistical difficulty in getting to Bulman and risk to the flight crew, it would be reasonable to delay the retrieval until daylight. He was retrieved in the morning to Royal Darwin Hospital where the path lab confirmed that there was no envenomation.
The Big Questions
So we’re left with questions that really matter (like all the best bits of research). My questions for anyone who wants to chip in:
Based on the apparently low morbidity/mortality associated with snakebite and low incidence of envenomation in our data, can we justify the frequently high risk (night) flying associated with retrieving the group of patients without clear evidence of envenomation?
Would it be reasonable to delay retrieval of patients of ALL patients with no clinical evidence of envenomation until the morning?
Who is shooting for that runway at night? Who is already planning what they’ll have for breakfast first?
Well the good news is this is an ongoing project, so I’ll be updating when we have a bit more information.
Notes:
This post arose from work presented at this year’s ASA conference. Here’s a bit more reading so you can go back to the sources.
One of the excellent things about retrieval work is the opportunity a clinician is presented with to try new things. Dr Alan Garner reflects on his recent experiences trying out a very particular branch of retrieval medicine – neonates and paediatrics.
I have recently had the opportunity to do some work with NETS in NSW due to some staffing issues they have had (completely outside their control). For those not familiar with NETS they are the Newborn and Paediatric Emergency Transport Service in New South Wales (NSW). They are busy too, moving about 2700 patients are year, and fielding calls and offering advice on perhaps another 1500. There are also some perceptions out there in New South Wales that NETS cases take a long time, a good part of which is spent in conference calls.
I am an old dog. It is more than 20 years since I passed my fellowship exam and I have never really had much exposure to neonates, particularly significantly prem ones. My ED practice is in a hospital with a high risk obstetric unit and NICU. These patients never come near the ED. So this has been a scary experience for me dealing with patients that might as well be aliens as they bear so little resemblance to what I know. NETS also has a few legends attached. Mostly of long phone calls and even longer jobs. I came to the job keen to see things for myself.
When they’re the scary sort of alien
Some of my colleagues from CareFlight who are also helping out on the NETS roster are paediatric anaesthetists in their non-retrieval life. The first solo NETS shift that any of us did was by one of my paed anaesthetic colleagues. She was sent to a neonate with severe meconium aspiration in a metropolitan hospital in Sydney. After intubation and ventilation on 100% O2 the baby had airway pressures in the 40s, an unmeasurable tidal volume and pre-ductal saturations of 80. I had nightmares that night wondering what I had got myself into and feeling completely out of my depth.
Despite my initial terror I still managed to front up for my first shift and discovered that my colleague’s patient was possibly the sickest NETS had moved all year. Slightly calmer now I have survived several shifts and thought it might be time to give the old dog’s perspective of the alien landscape I have found myself in.
Describing other planets
For all the adult retrievalists out there that dabble in some paediatrics i.e. people like me, let me try and explain what it is like. Imagine a service set up to do only interhospital transports of patients with respiratory failure. There would be lots of people with COPD and asthma, pneumonia and ARDS. For the first two groups you might spend hours at the scene stabilising a patient on NIV before feeling it is safe to move them.
This represents excellent care as we know that once they are intubated the mortality rises sharply. Same with the pneumonia and ARDS patients – good critical care at the referring site is what it is all about and may even include getting an ECMO team to them. There is absolutely nothing time critical about moving any of them and it would indeed be poor practice to attempt to move them too early.
Now if you have been able to imagine such a service, this is what the population that NETS transports is overwhelmingly like. There is rarely any time critical intervention waiting at the receiving hospital, and getting them stable for transport can take a very long time. Neonates with hyaline membrane disease are the absolutely classic example of the stay and play patient. Intubate them, give some surfactant then wait for it to work. This is excellent management for these patients.
And you also have to understand how physiologically brittle these little creatures are. Just give them a poke and their sats are 70% (you think I am exaggerating). You really want to be sure that you have some sort of stability before you start bouncing a patient like this around in a moving vehicle.
The smallest patient that I have moved was 950gms. The only reason that I agreed to do the move was the kid was basically OK and was being moved from a NICU associated with a paediatric hospital to one closer to the family’s home so that another baby that needed paediatric surgical input could be accommodated.
This baby was “well” with just some air running by high flow nasal prongs. However if you picked him up, he cried or you shook him about (in a moving vehicle) his sats were high 70s/low 80s. And this was a well baby by their definition. The nurse I was with did a fantastic job (thanks Charlotte!) and I did my best to not look like I was getting in the way.
Space and time
For those that think NETS take a long time then you just really don’t get the patient population they deal with. There is no urgent interventional cardiology or transport to stroke centres. There is no parallel in their alternate universe to these patients from the adult world. The closest they get is trauma patients. Trauma however is a tiny proportion of the caseload, and the trend is increasingly to non-operative management wherever possible anyway. I have been hoping to do a trauma case when I have been working for NETS as that is right in my comfort zone. However there have not been any for me to do. Rather it has been lots of prem and term babies, and infants with either respiratory issues or seizures. The one nagging question I have is how a system more used to steady movement of a patient springs into action when they really do have to push it along. A bit more time and I might get to see that too.
Not those sorts of alien but there is a link to phoning home sort of …
Connecting Across Space
As a team member I have also had the opportunity to listen in to a lot of coordination calls. NETS coordination is a bit of a legend in NSW and rightly so. With a NETS transfer everyone at both ends (and the retrievalists in the middle) is involved in the initial conference call, and often any update calls along the way. And they can be long calls. There is a big plus though everyone knows what the plan is and they own it.
Just last week I was visiting one of the paediatric trauma hospitals in Sydney and they were lamenting that this is sometimes not the case when the adult system was moving a severely injured child, where it’s always been the case that the retrieval team takes the job and gets on with the job. That’s just how it’s been for as long as I’ve been around. They did not know what was happening or when the child would arrive. This is never the case with the NETS system. Although this theoretically is supposed to be the case in the adult world too there are lots of instances where it just does not happen unfortunately (I take as a reference point this report).
People find it easy to point out flaws with their approach, but I think the NETS coord system has several strengths:
NETS encourage the concept of “there is no dumb question” for all the non-paediatric hospitals in NSW. NETS accept that they will field some silly stuff that should probably never have got to them so that they don’t miss any child who really is sick. For the low level stuff they patiently patch the caller in with the local paediatrician (sometimes in the hospital the caller is in) so that the local systems can manage the case wherever possible.
An extension of this is they look for the nearest solution to the problem and don’t assume that a call equates to a request for transport. Getting the right people involved locally can often solve a problem locally. Or the closest solution for the patient might be a service somewhere else like across a state border.
As they work at finding the best solution for the patient, all the players talk together to agree and own the plan. As I have already said, there is never any confusion about who is doing what on a case that NETS coordinate.
The nurses who coordinate the calls at NETS are actually moving babies themselves the day before and after. They know all the logistical and clinical challenges as coordination and transport are both part of the same job. It is notable that London HEMS has a dispatch system which works because the dispatchers are paramedics who work on the helicopter as part of the same job. I don’t think this a coincidence.
Retrieving Little Aliens Produces Other Big Challenges
If NETS has a weakness compared with the adult services it is perhaps the fact that not many of their cases are done by specialists except when they are coaching new registrars. Particularly on the neonatal front some of the babies are fiendishly difficult to stabilise adequately for transport (like the first case done by my poor anaesthetic colleague mentioned above). They really need a consultant neonatologist for these cases as they seriously stretch the capabilities of both the humans and machines (see below) involved in caring for them. Perhaps an unexpected bonus of the recent challenges in staffing will be a few extra specialists in the shift mix seeing as the whole team benefits from their experience when they’re online.
Another issue is the equipment. Across all age groups NETS currently have four different ventilators which is a bit of a nightmare for new registrars coming into their system (although the skill of the nurses is a big mitigator here). Over the years as they have added new lines to the roster to keep up with increasing demand, they have added just enough equipment to keep up without retiring any of the old stuff. Some of the ventilators date from the 1980s. Although they still work, you would not find a machine of that vintage operating in an intensive care unit anywhere in NSW.
Infants are a particular problem. They have some Oxylog 3000 +s but they just will not ventilate a child with an ETT less than 4.5mm diameter and they struggle with bigger kids too if they have any lung pathology. There are newer turbine transport ventilators out there that can deliver a 2ml tidal volume and also ventilate a 100kg 15 year old. One ventilator could do the lot which would significantly decrease the training burden and hence increase patient safety too.
It will take a cash injection to fix this I suspect and it is not just buying the ventilators. The neonatal systems and paediatric bridges will need modification to mount the ventilators and in the aeromedical environment that means engineering certifications etc. etc. No cheap fix here. I understand this is currently being investigated but it can’t come soon enough.
And a final comment on the staff. As I am doctor, I have not had the chance to work directly with many of the NETS doctors as the standard team is doctor/nurse. I have now worked with a number of the nurses though and have been really impressed with their professionalism. It should be obvious from the caseload that I have described above that the little details really matter with these patients.
Like all good critical care nurses the NETS nurses have just the right level of OCD to be obsessive about the stuff that matters, but not quite enough to drive you nuts. I have been impressed with the risk management approach and planning, like discussing best and worst case scenarios with appropriate plans for each on the way to every case.
For me this has been a real learning experience. I am still way out of my comfort zone but hopefully there is still room for a new trick or two from the old dog.
The image here is from the Flickr Creative Commons area (unaltered) and was posted originally by JD Hancock.
In the meantime, Alan can’t be the only one who has found something that really challenged them recently. Any stories to share? There are comments for that.


 If you start with a clean slate and optimally position bases for either population coverage or average response time, both models place bases to cover that part of the coast (see Figure 2). Hardly surprising. When we modelled to optimise the existing base structure by adding or moving one or two bases, the mid north coast was either first or second location chosen by either model too.
If you start with a clean slate and optimally position bases for either population coverage or average response time, both models place bases to cover that part of the coast (see Figure 2). Hardly surprising. When we modelled to optimise the existing base structure by adding or moving one or two bases, the mid north coast was either first or second location chosen by either model too.