Last time Jodie Martin, Flight Nurse extraordinaire dropped by she shared one of our most popular posts ever. Jodie returns with a little on the Top End experience of sepsis.
Time for a look at some remote medicine again.
CareFlight provides the aeromedical service for the top half of the Northern Territory (NT) in Australia. The area covered by the service is the same size as France but has only 160,000 people. And less vineyards.
As 115,000 of this population are in Darwin which is serviced by road ambulance services this leaves CareFlight to provide services to about 45,000 people in very remote and widely scattered centres, most of which are small Indigenous communities. The catchment area has only two rural hospitals which are non-referral centres with care otherwise provided in remote health clinics. Even then not everyone lives close to a rural hospital or remote health clinic. Some rural folk still have to drive several hours or even a few days to any level of health care. Access to health care is a real challenge when someone becomes sick.
The Top End of the Northern Territory may be sparsely populated with 0.2 persons per square km, but it has the highest incidence of sepsis in Australia and five times higher rates than those recorded in the US and Europe 1,2. It has been suggested that one of the reasons for the high incidence of sepsis is related to the higher Indigenous population in the Top End 2. The incidence of sepsis requiring ICU admission in the Top End of the NT for Indigenous people is reported to be 4.7 per 1,000. In the non-Indigenous population there are 1.3 admissions per 1000 people. When compared to the rest of Australia, the rate of admission to an ICU for sepsis is 0.77 per 1,000 2 with national 28 day mortality rates of 32.4% 1.
The Top End – Not Just Popular with People
Human-invading bacteria and viruses love the warmth and moisture of the tropics. To make things even harder, the Top End has the highest rate in the world of melioidosis, a very nasty pathogen found in the wet tropics of Australia. Melioidosis has been classified as a Type B bioterrorism agent by the Centre for Disease Control in the US and kills up to 40% of infected patients often from rapidly fulminant disease. However most sepsis is of the more common garden variety, but still causes severe, life threatening illness.

When you add the challenges of distance and retrieval times, meeting targets for sepsis treatment which are time-based would seem an impossible task. Given this, we were keen to review the retrieval of septic shock patients in our service to see what the outcomes are like and whether we could improve the process. The results have just been published in the Air Medical Journal which you can find here.
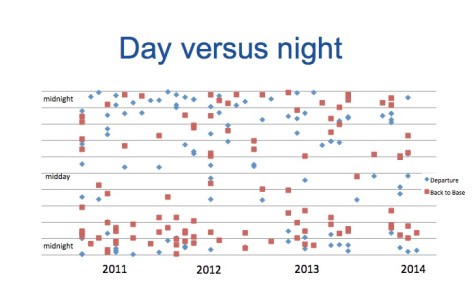
The patients were sick. A third of patients required intubation and 89% required inotropes. Median mission time however was 6 hours and the longest case took 12 hours. Given the remoteness and time delays inherent in retrieval over such distances with a population known to have worse health outcomes, you would expect mortality to be high. Surprisingly however the 30 day mortality in this group of 69 patients, which are predominately Indigenous, was only 13%. This is lower than previous rates described for both sepsis in Australian Indigenous populations and for patients in Australian and New Zealand intensive care units.
That’s Excellent, But Why?
It is interesting to speculate on the possible reasons for such good outcomes. Reasons might include:
- The relatively young age of the patients compared with many series. Perhaps the better physiological reserves of younger patients are still a key factor despite the higher rates of co-morbidities.
- Early antibiotics – these are almost always given by the end of the referral call. Good clinical coordination has a role to play in this too.
- Early aggressive fluid resuscitation – the median volume of crystalloid administered was 3L during the retrieval process.
- Inotropes administered following fluid resuscitation occurred in the vast majority of patients.
- Early referral – recognising when a patient is sick. This is something we’d like to gather more data on. We didn’t record how long a patient was in a remote health centre before a referral call was made, but we have a suspicion early referral might have played a part here.
It is also interesting to note the good outcomes that were achieved without invasive monitoring in approximately half the patients retrieved. Perhaps there are shades of the findings of the ARISE study here where fancy haemodynamic monitoring really did not seem to make much difference either – what matters in the retrieval context is early antibiotics, aggressive fluid resuscitation and early intubation when indicated.
We did not randomise patients to invasive versus non-invasive monitoring and it is possible that the sicker patients and those with longer transport times received the invasive version. But it is also possible that we get too hung up on this stuff and it is the basics that really matter whether you are in the city or a really remote health clinic.
The Wrap
The Australian Indigenous population have poorer health outcomes than the general community. Outcomes are even worse for those residing in remote areas than those in urban areas. In our small study it is pleasing to see such good outcomes despite remoteness and long retrieval times. Our young patient cohort recovered well considering how sick they were but what would be even better is preventing sepsis in the first instance. The incidence and burden of sepsis in young Indigenous people requires preventative strategies and appropriate and timely health care resources. Improving access to health care, improved housing and decreasing overcrowding, decreasing co-morbidities and decreasing rates of alcohol and tobacco use are hopefully just some of ways we can possibly decrease the incidence of sepsis and contribute to closing the gap.
Notes:
That croc with almost enough teeth came from flickr’s Creative Commons area and is unchanged from Jurgen Otto’s original post.
Here’s the link to the paper that’s just been published:
The two references with the actual superscript numbers above are here:
- Finfer S, Bellomo R, Lipman, J, et al. Adult population incidence of severe sepsis in Australian and New Zealand intensive care units. Intensive Care Med. 2004; 30: 589-596.
- Davis J, Cheng A, Humphrey A, Stephens D, Anstey N. Sepsis in the tropical Top End of Australia’s Northern Territory: Disease burden and impact on Indigenous Australians. Med J Aust. 2011; 194: 519-524.
Here’s a bit on melioidosis from the CDC website and here’s a review in the NEJM.
If you want to look more at the government’s Closing the Gap stuff, you could go here.