With a couple of new papers landing that touch on the issue of how you provide and measure quality care around airway management, Dr Alan Garner returns to point at big animals that are bad at hiding.
Two new airway papers have come across my desk in the last couple of weeks and I now wish I had waited a bit longer before putting up the last post on first look intubation as a quality measure.
So where to start? Well how about a place where everything is apparently big? Yes, there’s a bit of work just out of Texas which sheds further light on that first look intubation story so that’s where we’ll land.
Chasing Quality
It sounds like they have used RSI for a while but undertook a quality improvement project to try and reduce their peri-intubation hypoxia rate. The project involved introducing a bundle of interventions described in the paper as “patient positioning, apn[o]eic oxygenation, delayed sequence intubation, and goal-directed preoxygenation”.
The paper provides copies of the protocol for intubation pre- and post-bundle intervention in the on-line appendices so I might just go through them here to see what they did differently.
The first thing is there was an emphasis on positioning in the bundle, specifically head up a bit and ear-sternum positioning. Lots of goodness here that I strongly support.
The second measure they mention was apnoeic oxygenation. However looking at the pre- and post-bundle policies it is evident that they used it in both time periods. In the before period it ran at 6L/min till the sedation was given then it was turned up to 15L/min. In the post period however it was run at “MAX regulator flow” after the ketamine was administered. I don’t know about the O2 regulators in Texas but to me this does not sound like they changed anything significant. I will come back to apnoeic oxygenation later.
For pre-oxygenation in the pre- bundle period they used a NRB mask (with nasal prong O2 as above) in spontaneously ventilating patients (and arrested patients were excluded) but in the post- period the pre-oxygenation had to be by BVM with two handed technique to ensure a tight seal plus PEEP. More goodness here that warms my heart.
Delayed sequence intubation in this study refers to administering 2mg/kg of ketamine then maximising preoxygenation for at least 3mins prior to administration of the muscle relaxant. I don’t think this is necessary in all patients but this was the policy in the bundle.
The last thing they did was “goal-directed preoxygenation”. This refers to having a SpO2 target >93% for at least 3 minutes during the pre-oxygenation phase after the ketamine had been administered. If they could not achieve >93% the patient was managed with an LMA or BVM and transported. I think this represents sensible patient selection in that it removes the high risk of desaturation patients from the process. When you look at the results you need to keep this patient selection in mind. However I agree that in their system this is a reasonable approach to ensure patient safety for which the managers should be applauded.
Show Me The Money
Yes let’s get to that money shot:
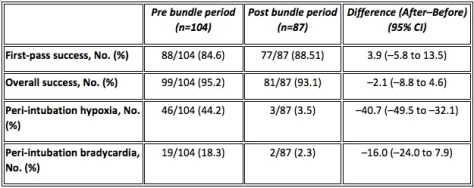
I have been banging on about peri-intubation hypoxia being far more important than first look intubation rate for a while now and this data shows really clearly why.
There is no significant difference in this study in either first look or overall success rates pre and post the bundle but the hypoxia rate fell by a massive absolute 41%! The 16% decrease in bradycardia emphasises just how much difference they made. The managers of this system and their staff alike both need to be congratulated for this achievement as this is something that really matters. And the first pass and overall success rates give no clue!
It really is time to drop first look as a quality measure and move on. You could look at this paper and start wondering if it might even be worth dropping overall success rate too, which is an interesting thought. Their policy favoured patient safety over procedural success rates by abandoning the attempt if the pre-oxygenation saturations could not be raised above 93%. It looks like it is working out well for the patients.
Oh, Back to Oxygenation
I promised I would come back to the apnoeic oxygenation issue. I know the authors state that it was part of their bundle, but it was used in the pre- bundle period as well. Hence there is no data here to support it’s use.
All three randomised controlled trials of apoeic oxygenation in the ED and ICU contexts (see the notes at the end) have now failed to find even a suggestion that it helps (check those notes at the end for links) and there are no prehospital RCTs. My take is that it is time to move on from this one too and simply emphasise good pre-oxygenation and good process when the sats start to fall – or never rise in the first place like this group did so well.
Overall a big well done to the Williamson County EMS folks and thanks for sharing your journey with us.
Moving Right Along
The other paper comes out of London, where the ever-industrious HEMS group have published a retrospective review of their database over a 5 year period (from 2009-2014). They were looking for adult trauma patients they reached with an initial noninvasive systolic blood pressure of 90 mmHg or less (or where a definite reading wasn’t there, those with a central pulse only) and with a GCS of 13-15.
This gave them a total of 265 patients (out of a potential 9480 they attended). 118 of those underwent induction of anaesthesia out there beyond the hospital doors (though with exclusions in analysis they end up with 101 to look at) and the other 147 (that number dropped to 135 on the analysis) got to hospital without that happening.
Now the stated indications for anaesthesia listed are actual or impending airway compromise, ventilatory failure, unconsciousness, humanitarian need, patients unmanageable or severely agitated after head injury, and anticipated clinical course.
Now given that the inclusion criteria includes patients having a GCS of 13-15, it seems like both unconsciousness and those really impossible to handle after head injury are likely to be pretty small numbers in that 101. Even airway compromise, ventilatory failure and humanitarian need seem like they’d be not the commonest indications in that list that would apply to this patient group, though they’d account for some.
I guess it’s possible the patients were all initially GCS 13-15 on the team’s arrival but deteriorated en route, though I just can’t sift that out from the paper. Plus if that was the case it seems like you’d say that.
The Outcomes
In their 236 study patients, 21 died and 15 of those were in the ‘received an anaesthetic’ group. The unadjusted odds ratio for death was 3.73 (1.3-12.21; P = 0.01). When adjusted for age, injury mechanics, heart rate and hypovolaemia the odds ratio remained at 3.07 (1.03-9.14; p = 0.04).
Yikes, sort of.
What To Make of That?
I guess we should make of it that … things you’d expect to happen, happen? Intubating hypotensive patients and then adding positive pressure ventilation in the prehospital setting is potentially risky for patients for a variety of known pharmacological and physiological reasons that the authors actually go into.
So the question is why embark on such a procedure where you know the dangers in detail? You’ve have to really believe in it to end up wiht 101 cases to follow up.
It feels like there’s an elephant in the room to try and address by name. I wonder if it has something to do with a practice I observed while working in the south-east of England 8 years ago. It relates to that last category “anticipated clinical course”.

The concept here is that if you figure the patient is going to be intubated later on in the hospital, you might as well get on and do it. Except the data here suggests that, much like you’d expect, you probably shouldn’t get on and channel your inner Nike marketing script.
Just because you can does not mean you should. This paper really drives this home though it doesn’t really seem to come straight out and say it. It does pass the comment that “Emergency anaesthesia performed in-hospital for patients with cardiovascular compromise is often delayed until the patient is in theatre and the surgeon is ready to proceed.” Perhaps the problem isn’t using the phrase “anticipated clinical course”. It might be that you just have to remember that the anticipated course might best contain ‘risky things should probably happen in the safest spot’ in the script.
Compare and Contrast
The process of undertaking emergency anaesthesia because later the patient might require emergency anaesthesia is pretty much the complete opposite of the approach from the Williamson County EMS folks. They erred on the side of patient safety and withheld intubation if it was associated with unacceptable risk.
This paper demonstrates that emergency anaesthesia in patients with a high GCS but haemodynamic instability is associated with higher mortality. We should probably be glad the authors have made this so apparent, because this is probably as good as we’re going to get. We’re not going to get a randomised controlled trial to compare groups. No one is allowing that randomisation any time soon making this another example of needing to accept non-RCT research as the best we’ll get to inform our thinking.
Patients with hypovolaemia due to bleeding need haemorrhage control. The highest priority in patients with that sort of hypovolaemia would seem to be getting them to the point of haemorrhage control quicker. And delaying access to haemorrhage control (because the prehospital anaesthesia bit does add time in the prehospital setting) when the patient has a GCS of 13-15 doesn’t seem to prioritise patient safety enough. Patients probably need us to adjust our thinking on this one.
That seems like common sense. The retrospective look back tells us pretty conclusively it’s a worse option for patients. And now it’s up to us to look forwards to how we’ll view those indications for our next patients. And “anticipated clinical course” probably just doesn’t cut it.
Notes:
That hovering elephant head was posted by James Hammond in a Creative Commons-like fashion on unsplash.com and is unchanged here.
How about all those things that got a mention above that you should really go and read for yourself?
Here’s that whole bundle of care paper out of Texas:
Those RCTs of apnoeic oxygenation in critical care environments mentioned are these ones:
And that paper on the hypotensive, awake prehospital patients scoring an anaesthetic is this one: