This is a post put together by Dr Andrew Weatherall as background preparation for a talk at the SPANZA Paeds Update from March 14, 2015. This is an update for the occasional paeds anaesthetist. It’s not about covering it all but hopefully there’s a few useful points in there to prompt a little thought and discussion.
For lots of people who do a bit of paediatric care, there’s a bit of nervousness around little people. It’s a bit disproportionate to the numbers of actual cases of course because paeds trauma is not common. In fact, rates are slowly going down.
There is also a common paediatric conundrum to deal with – what do you do with adult evidence? This is because overwhelmingly trauma literature deals in the bigger, smellier version of Homo sapiens.
So the challenge is to provide a refresher on something that is getting less common for most of us, using evidence for other patients.
This might be easier with a story, weaved from a bit of experience and not that much imagination.

The Call Comes In
You get a call from the emergency department that they are expecting a paediatric patient from a crash, not too far from your hospital out on the far edges of the city. The road speed limit is around 80 km/hr and they have a 6 year old child who was sitting in the rear right passenger seat, in a booster seat. He’s probably too small for this booster seat. It doesn’t look like he was well secured.
The child was initially GCS 12/15, with a heart rate of 145/min, BP 85/58, a sore right upper quadrant, and a deformed right upper leg. Initially SpO2 was 96% but is now 100% on oxygen.
Where Should They Go?
Of the schools of thought (big kids’ centre vs place where they do lots of trauma but not lots of kids), NSW has gone for the hospitals with the pretty waiting rooms.
Probably the most relevant local research on the topic is from Mitchell et al. who looked at trends in kids going to paeds trauma centres or elsewhere. They found kids getting definitive care at a paeds trauma centre had a survival advantage 3-6 times higher those treated at an adult trauma centre.
There are issues with this. Mortality as a sole marker when you’re only discussing about 80 kids across 6 years may not be the most reliable marker of quality care. You only need one or two cases to shift from one column to the other to significantly skew the picture.
Possibly the more significant finding was the delay created by making that one stop. Stopping at another hospital (even within the metropolitan area) delayed arrival at the paediatric trauma centre by 4.4-6.3 hours. Early discussions to transfer obviously need to become a priority.
In NSW, the policy is now for ambulance officers to go directly to the paeds trauma centre if it’s possible within 60 minutes. Unless they don’t think they’ll get there.
The impact on the doctor working outside the kids trauma centres is two-fold:
- There’s less paeds trauma to see.
- The paeds trauma you do see will be the bad stuff.
Great mix.

At Emergency
So the patient, let’s call him Joe, arrives. For the sake of discussion I’m going to assume he did come to the paeds trauma centre, but there’s a whole separate (possibly more interesting) scenario you could think through where he goes to a smaller metropolitan hospital.
Joe arrives with an IV cannula in place and Hartmann’s running. He has a hard cervical collar in place. His GCS has improved to 14/15 (he’s closing his eyes but he seems a little scared) but his heart rate is now 155/min and his BP is 78/50. Peripheral oxygen saturations are still 100% on oxygen (they were 96% off oxygen). He is sore and tender in his right upper quadrant just like they promised. That right femur does look broken. There’s also a lump on the right side of his head, towards the front just on the edge of the hairline.
The New Alphabet
We all remember the alphabet, whether first drummed in by the fluffy denizens of Sesame Street, or mostly embedded by a trauma course. A then B then C.
Anyone working in trauma knows this is only the older version. So 1900s. The trauma alphabet now has a bunch of variations (C-A-B-C, MH-A-B-C, choose your edit) to highlight the need to think about arresting blood loss early.
A lot of this shift in thinking is surely related to the vast amount of knowledge gained in managing trauma from military conflict where stopping haemorrhage is one of the most effective things you can do to save lives.
The causes may be different (especially in kids), but some of the thinking can be transferred.
This makes sense not just because bleeding is not great for patients. It’s also because many of the measures required to stop it take more than a couple of minutes. Not so much in the case of tourniquets or fancy dressings that make you clot. Things like surgery, or interventional radiology, or blood product management.
If you’re an occasional paediatric trauma practitioner, there’s a few points worth remembering if you’re going to elevate the importance of haemorrhage control, even while getting the other stuff done:
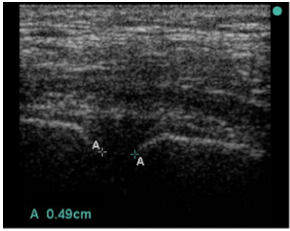
- Find the blood early – better rapid diagnostic options, particularly ultrasound, need to be deployed early to figure out where blood loss might be happening.
- Decisions need to support stopping bleeding – if the patient is bleeding, it is more than a bit important to progress continually towards making them not bleed. This is particularly relevant to arranging radiology and surgery as quickly as possible where indicated.
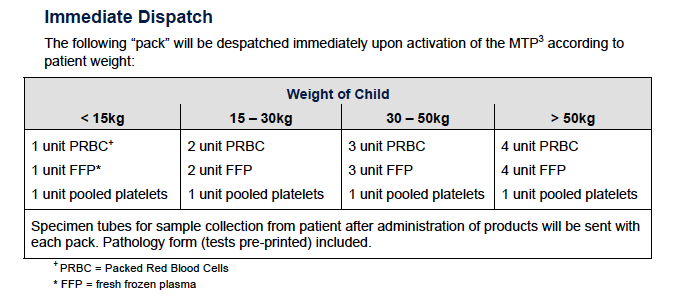
- Transfusion – bleeding patients don’t need salty fluids. They need blood. And given what we know about acute traumatic coagulopathy, they probably need it in a ratio approaching 1:1:1 (red stuff: plasma:platelets).
- Give TXA – after CRASH-2 and MATTERs, tranexamic acid has also made it to kids. A fuller discussion is over here (and there’s also the Royal College of Paediatrics and Child Health thing here though as I mention in that other post, I think they’ve got the doses not quite right).

Joe is Getting Better
Ultrasound confirms some free fluid in the abdomen. The fractured femur is reasonably well aligned but you’ve started warmed blood products early. Joe is responding to his first 10 mL/kg of products with his heart rate already down to 135/min and a BP of 88/50. Respiratory status is stable. GCS is 15/15 and you’ve supplemented his prehospital intranasal fentanyl with IV morphine.
You decide to go to the CT scanner to figure out exactly what is going on with the abdominal injury. Once around there Joe vomits and starts to get agitated. CT confirms a right front-temporal extradural haematoma. As he’s deteriorating you head up to theatres.

Now I’m going to assume anyone reading this is pretty happy with an approach to rapid sequence induction with in-line stabilisation to manage spinal precautions (not that we’d have a hard collar anyway, because those are on the way out in the draft ILCOR guidelines). We’d all agree on the need for ongoing resuscitation. I’ll also assume no one is going to stop the surgeons from fixing the actual problem while you mess about getting invasive arterial blood pressure measurement and a central line sorted.
What would be nice is some better evidence on what are the right blood pressure targets.
What BP target for traumatic brain injury?
Still, the best the literature can offer is a bit of a ¯\_(ツ)_/¯
If you look at this review from 2012 the suggestions amount to:
- Don’t let systemic mean arterial pressure go below normal for age.
- It might be even better to aim for a systolic blood pressure above the 75th percentile.
- If you do have intracranial pressure monitoring and can therefore calculate cerebral perfusion pressure, then aim for > 50 mmHg in 6-17 year olds and > 40 mmHg in kids younger than that.
Hard to escape the thought we need more research on this.
The Rest of Joe’s Story
Everyone performs magnificently. Joe’s extradural is drained. His femur is later fixed and his intra-abdominal injuries are managed conservatively. The next most important thing might just be that you remembered to give him good analgesia.
Not Forgetting the Good Stuff
I might have some professional bias here, but I think remembering analgesia is just as important as the rest of it. Studies like this one suggest surprisingly high rates of PTSD symptoms even 18 months after relatively minor injury (38% though it was a small study). Although the contributors to PTSD are complex there is some evidence (certainly in burns patients) that early use of opioid analgesia is associated with lower rates of PTSD symptoms.
This stuff matters. A kid with PTSD symptoms is more than just an anxious kid. They are the kid who is struggling with school, struggling with social skills and generally struggling with the rest of the life they were supposed to be getting on with. Pain relief matters.
So it is worth prioritising good analgesia:
- Record pain scores as a vital part of the record.
- Block everything that is relevant (no child with a femur fracture should have an opportunity for a femoral block of some description missed).
- Remember treatment as analgesia (don’t just leave the fracture like you found it, for example).
- Give rapidly acting,titratable drugs as a priority with regular checks of efficacy.
- For example, fentanyl 5 mcg/kg in a 10 mL syringe gives you 0.5 mcg/kg/dose if you give 1 mL at a time. Do this and reassess every 3 minutes.
- Likewise, ketamine 1 mg/kg in 10 mL provides a dose of 0.1 mg/kg each time you give 1 mL (though some would say you should use midazolam to offset dysphoria too).
- Don’t forget novel options – methoxyflurane anyone?
The Wrap
Paeds trauma may not be as common, but it needs to be done to the same high standards we expect of trauma care anywhere. Most of the stories in resuscitation are well worn tales. But there are a few things to really take away:
* Think about doing everything to stop bleeding early.
* More blood for resuscitation, but more sensibly too.
* Never forget pain relief.
And with any luck, most of this is already old news.
Postscript: Just after I put this together, the always excellent St Emlyn’s blog put up something covering the latest changes to APLS teaching. To my immense relief a lot of it is the same. It’s worth checking out.
After the postscript: This isn’t designed to be too prescriptive and everything should be figured out in local context. Obviously any thoughts anyone has to share would be very welcome.
![Come this way for other new thoughts but no more bad visual puns, people of the future. [Via Alan Kotok on flickr under CC 2.0]](https://careflightcollective.com/wp-content/uploads/2015/02/segway-copy.jpg)

!["Please, go on" says Public Holiday Numbat [unchanged via quollism on flickr under CC]](https://careflightcollective.com/wp-content/uploads/2015/02/numbat-copy.jpg)