
It is very exciting to introduce Tim Wallace, flight nurse from the Top End, on a topic sorely neglected for a website coming from Australia – animals that can kill you. Actually, perhaps Tim can introduce Tim.
“When I was a researcher working for a haematologist, I wanted to be a paramedic, but I ended up as a pedantic number chaser driving ventilators (ICU nurse). So I went to uni again so I could be a paramedic. Then I got this job and now I’m studying midwifery (I’ve been a uni student for 9 of the last 15 years). I came to Darwin then left after a couple of years and went rock climbing for a year with my now wifey. I thought the grass was greener down south. It wasn’t. I like Darwin. Finally, I think cats are the only malicious animal.
It’s 11 p.m. one night, in the middle of the wet season and a referral comes in for a suspected snake bite in Bulman. What? You don’t remember where Bulman is? Perhaps refresh your geography here.
Here’s the stuff you find out straight away:
- A 34 year old male has been bitten by something on the foot.
- He presented around 1 hour before the phone call with a story of walking along the road and stepping on a snake that then bit him. Bearing in mind that an Indigenous man from a very remote area like this is probably very familiar with the characteristics and behaviours of the local wildlife, this man says he didn’t see the snake, but felt it and has some marks on his left ankle that could be puncture marks.
- He walked to the clinic (1km) and since then has had the leg immobilised and a pressure bandage applied.
- His observations are unexciting and he is completely asymptomatic of any of the obvious signs (e.g. bleeding from cannula sites) or often subtle symptoms (e.g. abdominal pain) that might be associated with a snakebite.
So what do you make of a story like this? Well typically in a case like this a lot of emphasis is placed on the story as there are a lot of variables (and ambiguity) associated with confirming a snake bite and predicting the clinical course, including:
- What first aid has actually happened? Was it immediate or delayed, effective or ineffective?
- Timing: while a bite from a brown snake can be almost immediately obvious, death adder neurotoxicity may be delayed as long as 24hours.
- Syndromes of envenomation have very poor specificity in general (see ‘syndromes of envenomation’ table/picture)
- You often see dry bites where the snake digs in with the fangs but does not inject venom.
- Then there are stick bites, such as: did not see snake, but felt something while walking in the bush at night.
Let’s Talk Logistics
Back to our patient – how will we get there?
Bulman is ~550km as the Kingair flies and is exceptionally isolated and now has no emergency medical services (as they are all tied up with this case). The strip is unlit and not suitable for night landings. While it is possible to get in using the helicopter, there is a large band of storms between us and Bulman that means a bumpy marathon of a flight in what one of my colleagues calls the ‘vomitron’, stopping for fuel via a detour to the north of Kakadu on the way there and back.
Yeah. It’s not going to be easy.
Are the Snakes Dangerous?
Well everything in Australia is designed to kill you and the Top End is the most Australian bit of Australia. We have some awesome elapids (hollow fixed venom injecting fanged snakes) up here and snakebite is an increasingly common emergency presentation (as you will see from our data). Australia sees ~3 fatal snakebites per year + occasional significant morbidity (e.g. mechanical ventilation, neurological sequelae at discharge).
This is the only one I have seen in the Top End in the 5 years I’ve been here.
Most of the mortality is associated with the brown snake family whose victims classically present with a story of early collapse and go on to develop VICC (venom induced consumptive coagulopathy) and occasionally signs and symptoms of neurotoxicity. In the Top End, in addition to the western brown, the other problematic species are the myotoxic king browns (mulga snake), neurotoxic death adders and less commonly the mighty taipan (VICC, neurotoxicity). Many of our retrieval registrars come from countries with boring fauna and this topic is very exciting for them.


Having posed this scenario to a few of the retrieval consultants at CareFlight they all placed significant emphasis on how convincing the story was and all offered varying perspectives on the priority of retrieving this man. Remote clinics use the ‘CARPA Standard Treatment Manual’ protocols for managing emergency presentations, and CARPA is quite clear about snakebite:

And we can’t assume the RAN was comfortable by herself with this guy in her clinic.

Despite the rigid proclamations of the CARPA manual, I reckon there are unanswered questions about when (and if) patients who are suspected to have been bitten by a snake should be retrieved. As I have alluded to, confirming a diagnosis over the phone is difficult and a lot hinges on how convincing the story is. With this in mind we decided to try and arm ourselves with some hard facts, undertaking an audit of our retrieval database to quantify the existing situation around suspected snakebite retrievals.

Let’s Talk Numbers
Interestingly, the numbers of retrievals have increased somewhat since the last published data:
– Currie (2004) – 8.6 year sample – 13.6 aeromedical retrievals per year
– Our audit – 3.8 year sample – 30.2 aeromedical retrievals per year
Why? We’re just not sure.
When it comes to confirmed envenomation we get to a very select group:
– 3.5% (4 of 115 patients) – we’ve used antivenom twice in this period
The comparison? Well previously published data for northern Australia has quoted 5-23%.
Why are those numbers for confirmed envenomation lower in our stats? We don’t quite know that either.
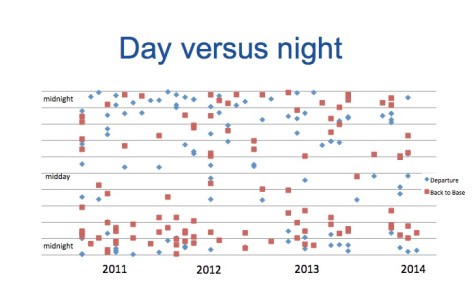
Then there’s the when – is there any particular time of day when the calls come in? Well ~65% of retrievals occur at night – see the slightly busy plot of night retrieval timings
Of course, the timing also has some implications for our pilots.
Flying High
In the Top End strips vary from well serviced, long, sealed, well lit and fenced in with GPS approaches (eg. Gove, Groote Eyeland) to poorly lit, narrow, occasionally dirt strips that are actually primarily the homes of kangaroos and buffalo and only occasionally used to land aircraft. The lights in many remote strips are solar, so they are great at 11pm but generally a lot less bright by 3am.
Crucially, many of these strips have no GPS approach. Where there is a GPS approach, the avionics aid the pilot in landing. Where there is no GPS approach, the pilots do a ‘visual circling approach’. What does that mean for safety? Well night flying is 3 times more dangerous than the equivalent aviation work in daylight hours. A visual circling approach is 25 times (!) more dangerous than a GPS approach. 25 times. (As a sidenote, helicopter EMS operations are also more dangerous at night.)
Perhaps the best insight for the aviation lay-person is to watch this video of a visual night time landing filmed by one of my colleagues on an after hours retrieval.
How were you planning to get there again?
Back to the Bitten
Back to our dude in Bulman. The retrieval consultant, in consultation with the logistics coordinator and flight crew decided that the the face of apparent low risk to the patient and massive logistical difficulty in getting to Bulman and risk to the flight crew, it would be reasonable to delay the retrieval until daylight. He was retrieved in the morning to Royal Darwin Hospital where the path lab confirmed that there was no envenomation.
The Big Questions
So we’re left with questions that really matter (like all the best bits of research). My questions for anyone who wants to chip in:
- Based on the apparently low morbidity/mortality associated with snakebite and low incidence of envenomation in our data, can we justify the frequently high risk (night) flying associated with retrieving the group of patients without clear evidence of envenomation?
- Would it be reasonable to delay retrieval of patients of ALL patients with no clinical evidence of envenomation until the morning?
Who is shooting for that runway at night? Who is already planning what they’ll have for breakfast first?
Well the good news is this is an ongoing project, so I’ll be updating when we have a bit more information.
Notes:
This post arose from work presented at this year’s ASA conference. Here’s a bit more reading so you can go back to the sources.
ATSB. 2012. Visual flight at night accidents: What you can’t see can still hurt you.
Isbister G. Snake bite: a current approach to management. Australian Prescriber. 2008;29:5.
Sutherland SK. Deaths from snake bite in Australia, 1981-1991. Med J Aust. 1992;157:740-6.
And, if you’ve made it this far, remember you might like to follow the blog and you’ll get an e-mail with each post.

Tim,
great article and as someone who loves aeromedical retrieval and venomous creatures I’m embarassed not to have written this myself.
On the subject of aviation safety I wonder how the helicopter stats will look like in a few years time once NVG has soaked into the system for a while…….
Well done on the article, I think it’s a valuable contribution.
Cheers
PB
LikeLike