So you’re out there somewhere and you really want to do a thing you think might help but you don’t have your standard kit. Can you adopt the lessons of Richard Dean Anderson and improvise? Mel Brown has you covered.
Okay, so I am guessing from the title of this post you have a good idea of my age….I am talking about the original MacGyver, not the new one. And for those of you that are too young to know who I am talking about…..MacGyver could improvise everything he ever needed from anything that was “just” lying around. I once saw him create an explosive device with little more than a pepper shaker and some foil wrapping off some chewing gum.
It is wonderful that we live in a world where most of the time we have access to all we need (and more), including our medical equipment. But what happens when you don’t have what you need (or don’t have enough of what you need) to treat your patient?
So in line with our series on “I wish I knew then what I know now” we are going to look at MacGyvering (improvising) arterial tourniquets and pelvic binders – two devices that we are all very familiar with (or if you’re not you can be if you go …
These easily reproducible techniques are certainly something I wish I knew about when I first started nursing…..and no, it wasn’t when Florence was around (although I am pretty sure she trained one of my lecturers).
Continuing with the History Theme
Did you know that arterial tourniquets have been around for a while now? In fact, the first combat commander to advocate the use of tourniquets was Alexander the Great – he based his decisions on the works of the medical researches at Cos.
However it wasn’t until 1718 that Louis Petit, a French Surgeon, developed a “screw device” that could be placed over blood vessels to stop flow. From the French verb “tourner” (to turn), he named the device “tourniquet.”
Elegant, non?
Improvised Arterial Tourniquets
One of the most important things to remember with any arterial tourniquet is that indirect pressure MUST be applied whilst the tourniquet is being applied. This will at least minimise if not stop the bleeding whilst the tourniquet is being applied…
Improvised tourniquets need to be at least 5cm wide to ensure adequate arterial occlusion can be achieved. Have you ever wondered why a shark attack victim that has had an improvised tourniquet applied to their bitten leg (usually via a surfboard leg rope) soon begins bleeding again after the bleeding was originally stopped? Well the theory goes that the initial narrow occlusion of the artery was enough to completely occlude the artery but as the pressure proximal to the point of occlusion builds up behind the narrow improvised tourniquet the arterial pressure is able to beat the tourniquet and the patient begins bleeding again. You need something applied over a wide area to get the job done.
So, what should we use? Firstly you need to find a windlass device that is thick enough and tough enough to withstand the pressure applied to it as you twist it to tighten the tourniquet (which can be up to 300mmHg of pressure). Some things (and only some, there would be more) that are readily available include:
A thick solid stick (not always ideal)
An indicator lever (probably not out of your own car)
A screwdriver
A tyre lever
A set of pliers
As for the tourniquet itself, what should be used? Some materials used with good effect include (but again are not limited to):
Triangular bandages (make sure these are the cotton ones and not the cheap paper ones)
Seatbelts (once again probably not out of your own car)
Canvas belts
Shirt sleeve (preferably with non-stretchy material)
Neck ties (not sure how many of these are around these days).
One of the issues with improvised tourniquets is the narrowing of the tourniquet at the windlass point. This can pinch the patient’s skin and make an already painful intervention more painful. The narrowing of the tourniquet material can also lead to greater damage to the underlying skin, muscles and nerves. Having said that I am not sure the alternative of death due to blood loss is ideal either.
I think many of us have spoken about how we could improvise an arterial tourniquet….but how do we actually do it? Let’s use the triangular bandage as our improvised tourniquet to discuss this in detail.
Ideally you want two triangular bandages – lay the first one along the arm or leg.
Wrap the second triangular bandage over the first and around the arm or leg and tie a knot or two.
Place the improvised windlass rod on top of the knot and tie two more knots to secure that windlass (note: if you can’t tie knots, tie lots).
Turn the windlass until the bleeding stops and then turn once more. Secure the windlass in place with the first triangular bandage.
If you forgot the first triangular bandage you can use gaffer tape (or equivalent) to secure the windlass in place.
It is important to still write “T” and the time of application somewhere obvious (maybe on the patient’s forehead would catch the eye) as you would for any arterial tourniquet. Obviously improvising is not ideal when compared to commercially available products. However, they are life saving for your patient when you don’t have the equipment that you need available.
Improvised Pelvic Binding
Improvised pelvic binding has been widely used throughout Australia by our Ambulance services for a very long time – I think most people would be familiar with pelvic sheeting. There’s some nuance around when pelvic binding may or may not be useful (just check out the posts here, here, here and here) but what do you do if you’ve made an assessment it is worth trying and you’re without your fancy gear?
Well we all go driving or hiking with sheets in our car boot (that’d be a trunk for our North American friends) or backpacks, right? I don’t think so, and I know I certainly don’t. So what do we commonly have on us that we could use? A jacket works well as an improvised pelvic binder. Let’s have a look at what this looks like:
Prepare the jacket for use. Use the arms as a width guide and fold it up like so.
Place the jacket under the smalls of the knees where there is a natural hollow.
Preferably with two operators seesaw the jacket up to the correct position over the greater trochanters.
Bring the arms of the jacket together and tie a knot.
Twist those sleeves until the required pressure is achieved.
Secure that knot (gaffer tape works again, or zip ties or equivalent).
You’re done. And maybe cold, but done.
Once again it is obvious that improvising is not ideal when compared to commercially available pelvic binders. However they are life saving for your patient when you don’t have the equipment that you need available. All interventions, whether improvised or not, must be continually checked for effectiveness – especially if your patient is moved.
Summary
It is important that as clinicians we understand how to use the commercially made equipment we have available to us. However, it is just as important that we know how to improvise life saving interventions as there will be a time when we won’t have our equipment (or enough of it) to treat our patients. This is a predicament that I certainly don’t want to find myself in. So let’s share what we know as shared knowledge is power. Or share what MacGyver knows because that is also power.
A bit more reading:
Those posts on arterial tourniquets and bleeding are here.
Sometimes it’s worth wondering if the things we hear, see and feel are quite as we thought they were. Dr Alan Garner has a look at your senses when you get into the chest and wonders whether it’s all as straight forward as we like to think?
Let’s start this post by stating right upfront that this is about chest wounds. If that is not what you were thinking then time to look elsewhere.
What I want to discuss is the clinical diagnosis of tension pneumothorax in the field. The reason for the discussion is that I believe it is way over-diagnosed. When I worked in the UK 6 years ago it seemed tension was being diagnosed frequently and the reason given was the sound as they breached the pleura with the forceps. As the patient was positive pressure ventilated at the time then the sound must have been air rushing out of the pleural space as their intrathoracic pressure was positive throughout the respiratory cycle right?
Remember how we can’t rely on the sounds involved in clinical examination in the prehospital environment because they’re too unreliable? Well I was being told this one was always right. ‘Always’ is a big word in medicine
I’m also aware of at least one case where a patient with a single epigastric gunshot wound from a low velocity weapon had intubation and then bilateral finger thoracostomies. The comment at the time was that the prehospital doctor, who no doubt went into it all in good faith, stated that at the time of the thoracostomies they found a pneumothorax on one side and a tension on the other.
However on imaging and surgery the projectile went straight back into the pancreas and nowhere near either hemithorax or the diaphragm. Indeed the only injuries identified to any part of the chest were the thoracostomy wounds themselves. Again an intubated patient so the intrathoracic pressure must have been positive right? If the lung felt down then it had to be a pneumothorax? And if there was a sound on breaching pleura it must have been a tension?
Clearly in the second case the signs were misleading so what is happening here? Let’s put aside for a second the challenges of the initial diagnosis of pneumothorax and focus on the feel with the finger and the sound to the ears. Could it be that some of the evidence we’ve been lead to believe tells us we’re dealing with a pneumothorax can mislead experienced, well trained clinicians?
Diving In
Perhaps I have done a few more chest drains than most. Partly that is due to more than 20 years in the prehospital space but I probably did even more when I was a registrar 25 year ago. I spent 6 months working for a couple of respiratory physicians and I put lots of drains (mainly for malignant effusions) in patients who certainly did not have a pneumothorax before I started. It was common to hear a noise as the pleura was breached as the air rushed in. But this of course was in spontaneously ventilating patients and that is different right?
Obviously we need to go back to the physiology to see what is driving the movement of air either into or out of the hole we have made to determine whether the sound we are hearing is air going in, or air going out.
Back to Basics
Transpulmonary pressure is the pressure gradient that drives normal ventilation. It is the difference between the alveolar pressure and the intrapleural pressure in the lungs.
Ptp = Palv – Pip. Where Ptp is transpulmonary pressure, Palv is alveolar pressure, and Pip is intrapleural pressure.
(If you’d like a little more on this the excellent Life in the Fast Lane has a bit on transpulmonary pressure here.)
Also it turns out that you can get a google preview of John West’s classic textbook on respiratory physiology. Take a moment to go and enjoy Figure 4-9 on page 59.
You can see from panel B (I meant it, go and have a look) that intrapleural pressure varies between about -5 and -8 cmH2O at the mid-lung level during normal respiration. It is always negative and that’s due to elastic recoil of the lung which is being opposed by the chest wall. It is less negative at the dependent regions of the lung (reducing alveolar size) and more negative at the apex (increasing alveolar size).
Let’s Add Air
In the situation of a small pneumothorax the air in the pleural space makes the intrapleural pressure less negative and the driving pressure difference for ventilation is therefore reduced. If the pneumothorax is completely open to the air such as with an open thoracostomy wound the intrapleural pressure is equal to atmospheric pressure, the elastic recoil of the lung causes complete collapse and ventilation by chest expansion is impossible – positive airway pressure has to be applied.
It is not the situation of the pneumothorax that particularly concerns me. If they are hypoxic or hypotensive and the patient has a pneumothorax the chest should be decompressed – a complete no-brainer. The question is why are good clinicians decompressing normal chests and thinking there was a pneumothorax or even a tension when there was not? Does the physiology lead us there?
Patient One
First let’s consider the non-intubated patient with normal respiration and no pneumothorax. This is the situation with the patients with malignant effusions I was putting drains in years ago. Here the alveolar pressure is never more than a cmH2O or two positive or negative. The intrapleural pressure however is -5 to -8 cmH2O. Therefore it does not matter what phase of respiration you breach the pleura, the pressure gradient between the pleural space and atmosphere is negative and air will rush in.
The gradient is bigger in inspiration when alveolar pressure is negative (and therefore the total pressure is around -8 cmH2O) and less negative during expiration when it is more like -5 cmH2O. It is however always negative. It does not matter which part of the respiratory cycle you breach the pleura, air is going to flow into the pleural space and the elastic recoil of the lung will drive it to collapse. If you hear a noise as I often did, it is air rushing in, the classic sucking chest wound. An iatrogenic one.
Patient Two
I don’t think anyone would have an issue with things so far. So let’s move on to the intubated patient who does not have a pneumothorax. I am going to assume here that there is not a lot of airway resistance in our trauma patient (which is not to say they don’t have underlying obstructive pulmonary disease, anaphylaxis to the induction drugs you gave or a clot sitting in a big bronchus/ETT) as it makes the discussion a bit easier to assume that resistance is minimal (futile according to the Daleks) and the pressure you are seeing on your ventilator gauge is largely transmitted directly to the alveoli.
Looking at our transpulmonary pressure equation, unless the airway pressure and hence alveolar pressure is higher than about 5 cmH2O then the gradient at the time you open the pleura means air is going to enter the pleural cavity. (If they have significant airway resistance this could happen with much higher airway pressures).
Just have a quick eyeball of this time pressure chart of a standard volume cycled ventilator with no PEEP (and a self-inflating bag will provide a similar though more variable trace). And I deliberately have no PEEP in this chart. PEEP is not likely to be the first thing we reach for in the hypotensive trauma patient we have just intubated where we are concerned about the possibility of a pneumothorax.
With normal lungs the peak pressure here is probably about 20 cmH2O. What proportion of the total respiratory cycle is the airway pressure (and hence the alveolar pressure in our patient with low airway resistance) likely to be below 5 cmH2O? If your little prehospital ventilator has a roughly 1:2 I:E ratio as most do, then the answer is most of it.
In other words unless you have PEEP of at least 5 cmH2O even in your intubated patient the transpulmonary pressure is negative for a good half of the respiratory cycle. During at least half the respiratory cycle, if you hear a noise as you breach the pleura you are hearing air rushing IN.
The elastic recoil of the lung is the reason that you feel the lung has collapsed by the time you pull the forceps out and put your finger in unless you have some PEEP in play.
Now I’m not saying there has never been a time when the air wasn’t rushing in. I don’t think much of the word “always” in medicine, remember? I’m just suggesting that what we know of physiology would argue that there is at least a solid proportion of the time where that transpulmonary pressure gradient is negative when you breach the pleura, which means that there’s likely to be a good proportion of cases where those “certain” clinical signs become less reliable.
For a demonstration of this with the mother of all open thoracotomies (in a cadaver) check out this video.
The cadaver is intubated, a “generous” pleural decompression wound has been created, and on each expiration the lung collapses right down unless PEEP is applied. And note the collapse is complete on each expiration.
As long as the thoracostomy is big enough to freely communicate with the air (and if you are relying on the open “finger” technique rather than putting in a drain it needs to be large or they may re-tension), when you put your finger in during expiration the lung will be collapsed unless there is a reasonable amount of PEEP splinting things open pretty impressively.
It will be collapsed whether it already was before you made the wound or whether it happened as you spread the forceps and made the communicating hole. The time between making the hole and getting that sense of lung up or lung down with the finger is ample time for the lung to collapse down. It seems like this particular clinical sign probably tells you nothing about the state of play prior to the wound being made.
So noises can be deceptive and feeling a collapsed lung just means that the lung recoiled as the pleura was opened. Can you even guarantee which phase of the respiratory cycle the patient was in when you made that hole? Unless you had at least 5 cmH2O (and maybe more) PEEP on at the time you breached the pleura neither of these signs necessarily means anything.
Maybe none of us can trust our big ears?
Now, what?
Again, I’m not really into saying things like “always” or “never”. What I’m suggesting is that there might be a lot more grey around these clinical signs than might first seem to be the case.
So how do you know if they had a pneumothorax? For me that is almost always by ultrasound now. I don’t know how I managed for 15 of those 20+ years of prehospital care without one. Sometimes of course the scan is equivocal and you need to make a call based on the signs you see and the condition of the patient but I find this to be very infrequent with a good high frequency linear probe.
And as for tension the hallmark is abnormal physiology, particularly blood pressure. If decompressing the chest fixes the physiology then they had a tension. If it does not then they had a simple pneumothorax – or none at all. Because the noise you heard as you breached the pleura may have been air either entering or leaving the building, hearing a noise does not help you either way. Was Elvis ever in the building at all?
Notes:
I had the brilliant Dr Blair Munford review a heap of the physiology here to make sure it matched up.
After that link to the LITFL bit on transpulmonary pressure again? Then go right here.
And John West’s masterpiece (well at least the page mentioned) is here.
That image of Nahni with the big ears was posted to the Creative Commons part of flickr by Allan Henderson and is unaltered here.
Oh, and in case you didn’t know the truly amazing John West, Adelaide boy made good, has recorded his whole lecture series for you to go and watch. Because when you’re in your 80s you’ll probably be contributing to medical education like that too, right?
At the recent Student Paramedics Australasia International Conference 2016 held in Sydney, Dr Andrew Weatherall was given the topic of “things paramedics can do to produce better long-term outcomes after traumatic brain injury”. This is a version of that talk modified for the blog.
This topic, that someone else came up with, gets it.
So much of the time in prehospital medicine we focus on things we measure in the first hour or so. The stuff we do before we hit the doors of the hospital. That fairly bogus ‘golden hour’.
Those things matter. But the big picture of trauma care isn’t the first hour. It’s the rest of the patient’s life.
Everything we do in the prehospital setting is really about whether they get back to what they were dreaming of doing. It’s not up to us what those dreams are. Your patient might dream of playing big time sport. They might dream of creating the world’s great collection of corn chips that look like ex-Prime Ministers. They might want to fly on the first trip to Mars (and almost certainly die of cancer because everyone seems to be forgetting about deep space radiation). When we care for them we sort of have to want their dream to happen for them.
So on the days when I get to hang out with paramedics instead of getting paid by the government to wear pyjamas and give drugs to kids, this is the aim. And traumatic brain injury is worth looking after well.
We could dive into traumatic brain injury by starting with a bunch of graphs from a physiology text. Let’s dive into something to make it relevant.
The Scene
This is the scene we’ll be going to. You’ll end up looking mostly at the patient who was driving the SUV. It looks like they had an initial collision, rolled over and then nudged up against the hatch that was veering off the road. Emergency services have been called by a passing pharmacy student who has done a First Aid course. They tried shaking and shouting and got no response. They thought about feeling for a pulse and they’ve found one.
This patient is clearly one who might have a traumatic brain injury (TBI). They could end up as one of the patients with moderate or severe TBI who lead to a cost to the system of around $8.6 billion each year. That comes from a report prepared for the Victorian Neurotrauma Initiative released in 2009. It estimated that for 2008 Australia would have around 1400 in the moderate TBI group and 1000 in the severely injured group.
And each one of those people doesn’t get back to their planned life. Some of them end up needing help with simple things for their whole life.
So this is the job and the clock started 5 minutes ago. What should we focus on? Is it all about RSI? Is it about early TXA? Is about the sort of stuff you need an advanced medical team for?
Well that could be the basis of discussion but we should start with a reality check.
If you look at the NSW Institute of Trauma and Injury Management report of the 2014 trauma database stats, there were 3458 severely injured trauma patients. 66% of the patients had an injury to the head. 3 of the top 5 severe injuries were subdivisions of subdural haematomas.
Of those arriving straight to a trauma centre, 80.4% arrived in an ambulance (vs 12.6% in a helicopter).
Even allowing for some of those ambulances having an accompanying advanced prehospital team, I think this grouping of numbers says something pretty significant: the vast majority of “big” trauma patients will get their care from paramedics.
This also means that if we want to save the most brain cells we should focus on making sure the patients getting those transports have the best possible care that those paramedics’ training can make happen. That’s more important across the population than the advanced team’s contribution.
There is a separate chat to have some day about trying to get advanced teams to the jobs where they might really help or the best way to do pointy end stuff. That’s just not the focus for this particular bit.
It does brings us to the first key thing that trained paramedics can do to improve long-term neurological outcomes – be there.
The nature of their training and their ability to focus on getting the vital things done and get moving means that paramedics will invariably lift the standard of care of the patient when they turn up and do their job.
Now exactly what they should do we’ll get onto in a bit but there will only ever be a small number of meaningful interventions to do for the patient so it makes sense to get it done as efficiently as possible and get moving. And of course while neurosurgery is mostly not an urgent requirement, about 1 in 5 patients will need some form of early head-cutter work. That 20% of patients really want professionals who are trained to make things move.
So it might seem like there’s not much meat on just saying “be there”, but I think it’s worth noting as we go that the standard way professional paramedics go about their business represents a step up compared to what was managed in the past.
Now that you’re there …
Back to the patient. When you get there, the patient looks to be in their mid-30s, is making breathing efforts and there is some air moving but it is fairly noisy respiration. Initial peripheral saturations read at 85% and the measured blood pressure of 95 mmHg is somewhere near what you would have guessed by palpating the radial pulse. The patient’s GCS is 7, the pupils are equal and reactive. A quick glance suggests the right femur looks like it’s adopting a more meandering course than usual on the way down to the knee.
So what should our aim be for these patients? What targets do we have that are the best evidence-based ones available?
Somewhat disappointingly we don’t have that much evidence for discrete targets. What evidence there is hasn’t really shifted much over the last couple of decades. Most of the stuff we do leans heavily on a general understanding of physiology as much as firm numbers.
But let’s focus on the numbers we do have. They’re based mostly on retrospective looks at info from big data banks. And the number to remember is 90. That’s the breakpoint because:
90% saturations is around 60 mmHg pO2 and we know that patients who have a reading below that value have worse long-term neurological outcomes.
90 mmHg is the magic BP number for adults – a measurement below this is associated with worse outcomes.
And these markers kind of make sense. We often think about the primary injury already having happened when we get to the patient and focus on avoiding secondary injuries which we view as discrete and separate extra insults. Add new injuries and you make the outcome worse.
It’s probably more accurate to say that the primary injury evolves over a number of hours. In that traumatised brain there will be excitatory neurotransmitters looking to party way too much for the cells to recover. There will be inappropriate triggering of cell death. Calcium will be getting places it shouldn’t and generally grabbing onto cell elements it should leave alone. Each secondary injury ramps up processes like these as they continue to evolve. It’s one of those times all evidence-based practitioners need to try and stop evolution from being a thing.
There are a few other things worth keeping in mind:
The brain is pretty simple in its demands. It wants oxygen and nutrients delivered.
Things that make blood flow decrease aren’t good (remember that the injury itself is quite likely to drop blood flow well below normal).
Intracranial pressure that is high isn’t great. It compromises blood flow.
Oh, and it’s also worth mentioning that there aren’t many things inside the head that we influence the volume of prehospitally:
There’s the brain tissue (and the associated fluid that goes with it).
There’s blood. Blood can be inside vessels which gives us some scope to manipulate how much flow is occurring. Occasionally it will be outside vessels and the vast majority of times that patient will get their definitive care at the hands of a neurosurgeon.
There’s CSF (which we have less influence over).
So if our aims are basic do we have to wait for advanced techniques to try and reach this target? Of course not.
This brings us to the second important “thing that we can do right now” – be basic.
Consistent delivery of basic measures has the potential to save huge numbers of brain cells. It’s more meaningful than waiting to try and develop the infrastructure and expertise to get more people doing advanced things like RSI.
The perfect example is impact brain apnoea. This has really only been described in any detail fairly recently by Wilson et al but there are accounts throughout medical history and the animal literature that describes a phenomenon of subjects forgetting that whole breathing malarkey in the immediate aftermath of trauma.
The suggested treatment? Open the airway and support ventilation. Those simple steps are meaningful.
They’re meaningful for all patients with TBI too. Which is why it’s worth getting back to the simple message of “A-B-C” which some sage once told us was as easy as “1-2-3”. Simpler than the transition to adulthood from child stardom if you were that individual anyway.
So let’s work through those simple little letters.
1. How’s your “A” game?
Well, is it anarchy?
Failure to do the basic bit of airway well is one of the commonest issues we see when welcome people training at the kids’ hospital. It’s such an important foundation though. So ask yourself whether you do the basic version of “A” well. Is your jaw thrust good enough to get those bottom teeth in front of the top teeth? Do you reach for adjuncts like oropharyngeal or nasopharyngeal airways as an aid? Are you quick enough to move to a two hand technique?
Most importantly do you make sure that you create a good seal with your mask? The value of a good seal is actually highlighted by work looking at pre oxygenation techniques. A colleague from CareFlight, Dr Chris Groombridge, did a nifty study with volunteers evaluating the maximum expired oxygen level you could achieve with different techniques. Anaesthetic circuit vs bag-valve mask (either alone or with nasal cannulae or PEEP valve or both) vs non-rebreather mask (with and without nasal cannulae).
And at the end of 3 minutes you still couldn’t beat either the anaesthetic circuit or the bag-valve mask with a well-maintained seal.
Hayes-Bradley et al did some work with a slightly different focus, evaluating the impact of nasal cannulae on pre-oxygenation with a bag-valve mask set-up or non-rebreather. Nasal cannulae helped only where there was a deliberately created leak in the seal.
Now you could take the line that it’s just pragmatic to assume you’ll end up with a leak. But why should we accept doing the technique anyway other than perfectly? Let’s focus on getting the seal right.
We’ve really taken that to heart at work, making the effort to maintain that seal throughout pre-oxygenation. It’s all part of ensuring that our focus on is on the main game – maximising oxygenation throughout the RSI rather than pushing on to the laryngoscopy and intubation step without optimising things up front. The brain wants oxygen more than it wants laryngoscopy.
That some prioritisation of the basic step of managing “A” well – perfect performance of basic airway manoeuvres, suction and use of adjuncts – can apply to all of us, whether we intubate or not. It’s the first step to delivering on our first aim – get those peripheral saturations above 90.
It also feeds seamlessly onto …
“How good are your “B” moves?”
Is it carnival material?
What about those patients who need support for the breathing part of the equation. That might be via that bag-valve mask set-up or you might have supraglottic airways as an option you’ve been trained to use.
The question here is not just how well do you do it but do you take steps to make sure you’re using that skill set in the best interests of the patient?
So if you think a supraglottic airway might be appropriate for a patient do you quickly assess if they’re ready for it with a firm jaw thrust and a deep suction before placing it? Do you check what the seal is like once it’s in?
And how do you measure your effort with the bag you hook up to that SGA? Because it’s easy to puff away like your hand is a talking sock puppet. We should really all be hooking up capnography wherever we can (for bag-valve mask work too). It might not provide a trace like the intubated patient but it will be more accurate than a guesstimate. And without having a sense of where you’re at with the CO2, how do you know if you’re not creating hypocapnoea when hypocapnoea is associated with reduced cerebral blood flow (and of course hypercapnoea could cause raised ICP)?
Doing the “basics” well requires a bit of attention. Who knew?
But you might well say, what about RSI? Shouldn’t we be figuring out how to train people to do that? Well while there is a probable role for RSI it is really hard to demonstrate the positive benefit. That is probably partly because prospective research in prehospital medicine is very hard. But the evolution of the research that’s out there suggests that getting that high stakes procedure done well enough to have the benefit outweigh the potential complications will take a very long and concerted effort.
Take for example just 3 studies:
The San Diego RSI paper – this suggested worse outcomes but subsequent analysis revealed performance of the procedure with significant periods of hypoxia (57% of those analysed had a desaturation with an average time of 160 seconds and a median fall in saturations of 22%).
HIRT – which took long enough in recruitment that the system changed all around it, rendering it very difficult to keep arms of the study in their planned arms. Those that received the advanced interventions team as intended did have a 14% reduction in mortality but it’s not robust enough to bank your house on.
The Victorian paramedic RSI paper – this showed benefit but there were more patients in the control group lost to follow-up and you’d think that those who did better would be the ones you’d lose. Just one different outcome in the control group would have made the findings insignificant. So it’s not robust enough but for different reasons.
So RSI makes physiological sense and most would still say it has a role. But it’s hard to make it pay off. We can all do the basics right every day from today.
What should we see when people are doing “C”?
It’s not like there’s some study out there saying “this particular prehospital intervention related to circulation and haemorrhage leads to better TBI outcomes” but we can focus on maintaining that blood pressure above 90 mmHg. So things that cause catastrophic hypotension (say, pneumothorax with haemodynamic consequences) need treatment with whatever the provider is trained for.
If there is external haemorrhage that has to be controlled so we can focus on doing that particularly excellently. If you’re putting on a tourniquet, think about providing proximal occlusion of flow first with your whole weight (e.g. a knee not just into the groin but leaning in and twisting a bit to really slow down flow before the tourniquet goes on). Really provide pressure to stop bleeding if pressure is the treatment you’ve chosen. Splint that femoral fracture to reduce loss of blood volume.
At the same time it’s worth noting that some of the evidence base for things we do is less strong than we might assume. As covered by Dr Alan Garner in the series starting here, the evidence base for pelvic splints improving haemodynamics isn’t based on huge reams of work.
Other options will probably come through for lots of practitioners soon. Haemostatic dressings or granules are likely to make a difference for some patients. With a little more evidence TXA might roll out across the land. And while there are very interesting concepts like prehospital REBOA out there to be wielded by a select few, something like the Abdominal Aortic Junctional Tourniquet might be a far more significant option on a population level. Judicious use in the exsanguinating patient with due regard to the potential downsides (particularly if it might take a while to get to somewhere else) could be an option for an awful lot more practitioners.
The Other Simple Things
That’s not the end of the simple things of course. Think about whether you can sit your patient up to drop the ICP. Is there a better way to maintain C-spine stability then a rigid collar? Is there anything constricting the neck?
Add a lot of simple steps together and you have pretty comprehensive efforts for those brain cells that just want blood to flow and nutrients to turn up.
The Group Who Doesn’t Get the Simple Things
And while we’re at it, there is one group who tend to get much less of all of the things, including the basics.
Kids.
Which is not great if you’re trying to think about how to provide better long-term outcomes. Their long-term is even more long-term.
Bankole et al provide just one example of a study demonstrating this. They looked at prehospital care around a New Jersey centre and compared the care received by kids with TBI to that received by adults. The numbers are pretty stark (though some of the headline items relate to interventions like intubation).
69.2% of the kids intubated had complications at intubation. 20% of kids with a GCS under 8 had no attempt at intubation. Failed intubation rates were 29.03% (vs 2.27% in adults). Kids also had higher rates of the dislodgement, oesophageal intubation, wrong size of tube choice and a requirement for multiple attempts.
Even intravenous access was placed less (adults had a prehospital cannula 85.9% of the time whereas in kids with the same spectrum of pretty severe injuries it was 65.7%).
More recently advanced practitioners in Switzerland published around the topic of advanced airway management in kids and while they did well initially, wrong tube sizes and wrong depth of the tube turned up again.
There are lots of reasons we do less well with kids. We see them less for a start and there can be additional scene distractions. But ultimately we need to recognise this and figure out a way to make sure we step up to the mark.
Back to the Scene
The patient has been making respiratory efforts but you can see the chest see-sawing a bit with diaphragmatic effort with an added breathing buzzsaw soundtrack. You jaw thrust and the airway improves. A suction improves the airway still further. You add a bag-mask set-up and really focus on a great seal. The saturations rise above 95%. The femur looks like it’s taking a meandering the scenic route towards the knee but it’s soon splinted and a big wound in the calf gets pressure to slow the bleeding. You’re on your way…
Now that sounds pretty easy. When you’re in a lecture theatre or reading a lesser known blog it sounds even easier. But we all know that the scene isn’t actually that easy. We’re assailed by all sorts of things and there is plenty of work in simulation sessions (like here) showing that when faced with high stress situations we tend to omit things we ordinarily wouldn’t, do things we’d normally not contemplate and remember all of it less.
This touches on the next thing prehospital practitioners have to do to provide better care for the brain – be the same with your care, everywhere. (The astute reader will notice that not only did I match the formatting to the other “be” statements, I made it internally rhyme. I’m really trying to make it seem meaningful.)
Beyond starting by acknowledging the risks of a deterioration in performance depending on the day or the job or the other stuff in our lives, we have to figure out how to be consistently excellent with our care. That’s what the patient expects. Their brain cells aren’t very interested in your back story or your motivation. They’d like you to do your job.
The strategies to try and make sure you always step up are way too many to go in right here, so it’s worth looking around. But use the team, communicate well, share your plans with those around you, use checklists or practice tactical breathing or other focus techniques or whatever it is that works for your good self.
Just don’t accept that you have to be a hostage to all those other factors.
And part of not accepting the status quo is striving to always provide better than we can do right now. That requires all of us to be a leader.
If we want to be able to provide capnography for all those patients whose A and B we’re managing then we might need to advocate for that. If we want to be able to look back in detail at how well we did, then monitors that only store information every 2 minutes (which is so often the case with prehospital monitors) aren’t up to scratch and we need to lead those demands. We need to provide leadership in governance and education to keep our standards constantly improving. We might even need to advocate solutions to issues in other areas of health that would free up paramedics to be out on the roads so they can work on that being there bit.
Future Dreams
While this topic is mostly about what we can do right now we obviously have to keep an eye out for what comes next. And I could well be wrong but my guess is that the thing that comes next that makes a big difference across the population to those who suffer a TBI won’t be one of the magic bullets being tried like progesterone, or EPO, or even TXA.
What would be really great is to actually know what the brain wants right now. Is the blood pressure of 100 mmHg actually adequate for this person’s brain or are they usually hypertensive and critical cerebral ischaemia is being added to your mix?
Does this patient actually need their CO2 a little higher than you might have thought because blood flow isn’t so great? Is their evidence of haematoma developing on one side that hasn’t shown up clinically?
That’s part of why we’re researching tech like near-infrared spectroscopy tissue oximetry. Now I’m not convinced that particular technology will provide that information reliably enough, but I do think that the most meaningful thing we could add to prehospital TBI care is more info about what this patient’s individual brain would like, rather than being stuck with population-based gross numbers.
And if we find that device the ultimate result will probably be that it tells us how to do the basics just that little bit better for this particular patient.
Because they might have big plans for corn chips that look like ex-Prime Ministers.
Notes:
OK, this was a really long post, but when you put a talk into post form it can be like that.
Here are just a few things from along the way you might like to go and look at.
Oh, and I put stuff over on the blog site at www.songsorstories.com relating to kids anaesthesia. If you look at the categories “airway” and “tips and tricks” and “cannulation” you’ll find some basic tips for working on things.
All the images here are from flickr creative commons and unaltered.
Did you scroll this far? Well you will inherit the earth that is constructed where scrolling is rewarded. Here, have this porcupine reviewing pumpkins as payback.
Dr Alan Garner has a blog post in the context of a report just published. A catastrophe during a winching operation highlights the physiological challenges we sometimes add in the work we do.
The death of a patient during a winching incident in Victoria in 2013 was distressing for everyone concerned. I was asked by the Victorian Coroner’s Office to provide an expert opinion on the death based on some previous research I had conducted with one of our registrars, Dave Murphy, looking at the effects on respiratory function of various methods of helicopter rescue. I’m pretty sure at the time we were the only group in Australia who had published in this area so I guess we were the obvious choice.
As part of trying to avoid a similar incident the coroner’s office agreed to us publishing the case in an appropriate scientific journal so that operators worldwide would benefit from the lessons learned rather than just the industry in Australia. That report has just been published in Aerospace Medicine and Human Performance and can be found here.
The details of the case are now on the public record in both the coronial inquest and the ATSB investigation. Our case report focuses more on the physiology of hoisting than either of these forums needed.
For those not aware of the case the brief version is that a man of approximately 60 years of age and BMI of 45 with borderline cardiac failure injured his ankle whilst on a hunting trip in Victoria about a kilometre from the nearest road. Carrying him was considered risky for the rescuers (the terrain was steep) and a hoist extrication by helicopter was organised. An accompanied single sling technique was utilised.
Unfortunately as they approached the aircraft skid the patient became combative and then unconscious. He slipped from the strop despite the best efforts of the paramedic and crewman and fell to his death. I can only imagine the distress of the crew when this occurred.
The actions of the crew on the day were consistent with their company/Ambulance Victoria procedures and were within the specifications of the equipment utilised. They were just doing their best to provide their best care as they’d been trained. Neither was any of the equipment found to be faulty. The obvious question then is why did the fall happen?
What happens when you put someone in that hoist?
You need to go looking in the climbing literature to find the physiological effects of suspension with chest compression which is what happens when you are in a single strop. As you would expect, there is a constrictive effect upon respiration but there is also a considerable decrease in cardiac output resulting from the decreased venous return with raised intrathoracic pressure. The decrease in cardiac output has been demonstrated to be as much as a third in fit young climbers. The decrease in respiratory function parameters is similar (in both the Murphy paper and the one referenced in the link in the previous sentence).
When you think through what’s involved, the physiology makes sense.
Given that the chest compression associated with hoist rescue is of short duration it is generally adequately tolerated long enough to complete the rescue in fit young people. Having said that one of the best studies of the physiological effects of suspension in a chest harness was precipitated by the death of a 25 year old soldier who was left suspended in a single strop for just 6 minutes. Cardiovascular collapse can occur surprisingly rapidly. The man in the Victorian incident with his significant comorbidities was however not able to tolerate even a short period of thoracic compression and rapidly became unconscious.
The effects of single strop rescue in people who have been immersed even where they are otherwise fit and young is perhaps better known and the second sling under the knees (or hypostrop as it is often called) is in widespread use in this situation. For winches of non-immersed persons it seems that the physiological consequences of various rescue techniques are not well known in the industry however.
Subsequent actions by Ambulance Victoria, the helicopter operator, the Victorian Coroner, CASA and the Australian Transportation Safety Bureau (ATSB) all rightly concentrated on determining how a repeat of the incident could be avoided by better educating both clinical and operational crews about the physiological implications of hoisting techniques.
What are the options?
We have previously published on the use of the Coast Guard Rescue Basket due to its benign effect on physiology compared with other techniques (Murphy). It remains a surprise to us that this device is not in more widespread use. Ambulance Victoria has now introduced a sit type harness which is definitely to be preferred in hoists over land. The Rescue Basket can be used in winches out of water as well and we think is the more flexible option.
You can see that this sort of option would be easier on the physiology.
Should the single strop technique be banned entirely? We don’t believe so. Every rescue is a balance of risks and sometimes the risk to either the patient, aircraft or both means that an immediate single sling extrication may be the safest option overall. We certainly have not banned its use within CareFlight. Knowing about the physiological downsides we have discouraged its use for many years and encouraged use of the rescue basket. We have not removed it from the armamentarium however. If a crew elect to use it they have to provide a report in writing to the chief pilot about why they chose that technique. Knowing that there is that little bit of extra documentation required is enough to make teams make sure they’ve covered their options and risks carefully before they go ahead, but the option remains on the table.
Hoisting is risky for lots of reasons. We train for a range of safety considerations. And equally we have to make sure we’re aware of the physiological changes we might inflict on our all important patients.
Conflict of Interest Statement:
Neither I, nor either of my employers have any interest, financial or otherwise, in the manufacturer or distribution of the Coast Guard Rescue Basket.
Notes:
The first image here is from the Royal Navy Media Archive while the second was posted by Jim Howard, both to the Creative Commons area of flickr. Both are unchanged.
Continuing the series of sharing Carebundles, Alan Garner moves on to go through the stuff to include in multiple blunt trauma.
OK, part 2 in our Carebundle series. This time we will take a look at our multiple blunt trauma bundle. This excludes isolated head injury which we dealt with in the previous post. Why that order you may ask? Our Sydney service started life as a trial evaluating the management of severe head injury so TBI is front if mind for us. It is also more straightforward as there are not the competing priorities that occur in multiple trauma. And in the end we don’t just want survivors but neurologically intact survivors so starting with TBI and brain resuscitation makes sense. The multiple blunt trauma bundle has conditional targets that are modified by the presence or absence of brain injury acknowledging that brain resuscitation is our major goal.
So multiple blunt trauma is next. This has many bits of intrigue to it. It is multiple. We’re moving into the bits of the body where the pathology can be buried in the large splodgy bit in the middle. The diagnostic stuff can be pretty challenging at the side of the road. Oh, and because it’s multiple there’s always that threat of a new competitor emerging in the pathophysiology parade.
We won’t touch on penetrating trauma, burns and immersion all of which have their own bundles of joy for another time.
The Common Touch
All of the mandatory items overlap with the TBI bundle so we won’t waste any time on them here:
Venous access – yes we reckon that still makes sense.
Analgesia – opioids/ketamine – yes we’re really trying to stress that analgesia is a vital component of care, pretty much every time.
Monitoring: SpO2, NIBP, ECG
Spine immobilisation – note we’re just sticking with immobilisation.
SpO2 > 93% by ED arrival
Scene time < 25 min – again, this isn’t always possible which is part of why Carebundles provide guidance but need clinician judgment on each job. What we’re aiming for is a background enthusiasm for keeping momentum throughout the time we’re looking after patients so we can get them to the hospital with all those eager people waiting.
Transport direct to trauma centre – this would be the house for the eager people.
The conditional items however vary from the TBI bundle and we will now go through these.
Checking the Terms and Conditions
Long bone fractures splinted
There is no evidence I am aware of that this changes outcome but it is standard ATLS teaching and makes pain control easier. We carry lots of excellent drugs and the Carebundle makes a point of mentioning them but everything is easier if you manage the physical elements contributing to the painful situation. Really this is the original multimodal analgesia. It’s just that one of the modes is “physical things that stop hurting things from exercising a right to freedom of movement”.
Massive external haemorrhage controlled
There is strong cohort level data that this saves lives, although more so in the penetrating trauma context where it is more common. Certainly data from recent conflicts supports this as a primary aim of prehospital care. So we’re carrying tourniquets, dressings, chitosan gauze and granules (though the latter are more for penetrating wounds).
Right here seems to be a point to salute the wondrous quality of the shells of prawns.
TXA if episode of SBP < 90mmHg, or below normal for age
CRASH 2 inclusion criteria were felt to be a little vague to include in our bundle. After all the inclusion criteria in this study was any trauma patient who was at risk of haemorrhage. To make the bundle we felt the item needed to identify the cases where TXA really should have been given because the risk of life threatening haemorrhage is so high. There is some evidence that just a single episode of documented hypotension is enough to identify a group of very high risk patients so we adopted this as our criteria. As another mental trigger point, some of our team have expressed a process when they consider packed cell transfusion – “If I’m reaching for blood, I should reach for that drug.”
If shocked, SBP at ED arrival (refer fluid guideline)
No head injury: palpable central pulses/obeying command
With head injury: Palpable peripheral pulses, or SBP > 90mmHg / lower limit of normal for age
In setting our blood pressure targets we differentiated between those with and without head injuries. Without a head injury permissive hypotension is our strategy. With a head injury we adopted the lowest level identified in the Brain Trauma Foundation Guidelines i.e. SBP of 90mmHg as our target. This is lower than our target for isolated severe TBI where our target is a MAP of 90mmHg or SBP of 110mmHg (see the TBI bundle post for further details). That last modification is obviously for paediatric patients where the guidelines are a little harder to attach specific numbers to.
If GCS < 9:
Intubation and mechanical ventilation
EAM above JVP (head elevation)
ETCO2:
30-35mmHg if no chest trauma/shock
25-30mmHg if chest trauma/shock present
This is similar to our isolated severe TBI bundle but we finesse our etCO2 targets in the presence of other injuries that might affect the gradient between arterial and alveolar levels. There is some evidence that adopting a lower prehospital etCO2 target in patients with chest trauma and/or shock is reasonable as these patients have predictably higher gradients. My own personal experience is that in patients who have both chest trauma and shock the target needs to be even lower. I have achieved an etCO2 by ED arrival in the mid-twenties in patients where both these factors are present only to find the first blood gas reveals an arterial level in the 50s. I would certainly be interested in hearing other people’s experience on this one. Of course in our rapid response urban trauma work we don’t carry a POC blood gas analyser like we do in our interfacility transport operations. Actually measuring the arterial CO2 would be ideal but we don’t think this is practical for both time and weight reasons in our urban response service.
Thoracic decompression if hypoxic/shocked & clinical or US suspicion of pneumothorax
I don’t think this one is rocket science. Even if we know a pneumothorax is present on ultrasound we usually leave it alone if they are not compromised. If compromise is present however then we expect it to be decompressed.
If GCS <13, BSL documented
All patients with an altered level of consciousness get their blood glucose documented.
Pelvic binder if shock and:
possible AP compression / Vertical Shear injury or signs of pelvic #
We don’t expect pelvic binders to be placed prophylactically. There is no evidence to support such a practice. We do however think that binders are helpful on AP compression and possibly vertical shear type injuries and the patient is shocked.
So that is it for our multiple blunt trauma bundle. It’s what we came up with on a review of the evidence but we’re always open to clever thoughts from others. If you have comments or suggestions we would love to hear from you.
And next time we return to the Carebundles it might just be time to get to the pointy end of penetrating trauma.
Notes:
As always, we’re very happy to hear other people’s clever takes on things that are worth doing. It helps us re-examine our thinking.
Here’s the PubMed link again for the “a single low blood pressure” matters paper linked above:
Sometimes really simple questions don’t get asked. Here’s a joint post from Alan Garner and Andrew Weatherall on places you end up when you ask simple questions about ways of warming blood.
Carriage of packed red blood cells (PRBC) by HEMS crews has become increasingly common in the last several years in both Europe and North America. CareFlight was an early adopter in this regard and has been carrying PRBCs to prehospital incident scenes since the 1980s. We reported a case of a massive prehospital transfusion in the 1990s (worth a read to see how much Haemaccel was given before we arrived on the scene and how much things have changed in fluid management). In that case we tried to give plasma and platelets as well but the logistics were very difficult. This remains the case in Australia with plasma and platelets still not viable in a preparation that is practical for prehospital use.
Returning to the PRBCs however the issue of warming them was something that always vexed us. We experimented with a chemical heat packs in the late 1990s and early 2000s but could not find a method that we felt was reliable enough. We also looked at the Thermal Angel device from the US when it appeared on the market nearly 15 years ago, but as the battery weighed the best part of 3kg we decided that it still had not reached a point where the technology was viable for us to be carrying on our backs (battery technology has moved on a long way in the last 10 years and Thermal Angel now have a battery weighing 550gms).
Fast Forward
Hence we were pretty excited when we found that there was a new device available in the Australian market, the Belmont Buddy Lite, where the whole set up to warm blood or fluid weighs less than a kg. We have been using the device for 3 years now, and our clinical impression was somewhere between impressed and “finally”.
Still, one of our docs, James Milligan, thought it worth validating this new technology. Part of that was about checking that the machine does what it says on the box. Is it just marketing or is it really that good?
The other thing we wanted to assess was how a commercial device compared to all those old techniques we were once stuck with. Traditional methods used by EMS in our part of the world include:
Stuffing the unit under your armpit inside your jacket for as long as possible prior to transfusion.
Putting it on a warm surface (black spine board in the sun or bonnet of a vehicle). Yep, baking.
That chemical heat pack method we had tried 10 years ago.
Some things aren’t a prehospital option. Well this isn’t anywhere maybe.
The Nuts and Bolts
Now, how would you go about testing this? The first thought bubble included a pump set, a theatres wash bowl and a standard old temperature probe that you might use at operation. Oh, and some blood. Like most bubbles that don’t involve property, it didn’t last long.
So we were left with a question: how do you try and set things up to test a system for the real world so it is actually like you’d use it in that real world, while still allowing measurements with a bit of rigour? How consistent are you when you deploy a blood-giving pump set?
Enter Martin Gill, perfusionist extraordinaire from The Children’s Hospital at Westmead. Because when we thought “how do we test prehospital blood warmers” obviously we thought about heart sugery in newborns. We turned to Martin with the following brief:
We want to test prehospital blood warming options.
We want to measure temperature really well.
We’re keen on being pretty rigorous about as many things as we can actually. Can we guarantee flow rate reliably?
We figure we could use units of blood about to be discarded and we want to be able to do the most with what we’ve got. So we want to be able to use a unit for a bunch of testing runs.
And Martin delivered. He designed a circuit (check the diagram) that would guarantee flow, measure in 3 spots, cool the blood once it had run through, and run it all through again. There are some things you could never come up with yourself. That’s just one.
It looks a little different in three dimensions but you get the idea.
You might wonder how hard is it to get blood? Well actually it was pretty easy (thank you Sydney Children’s Hospital Network Human Research Ethics Committee and Haematology at The Children’s Hospital at Westmead).
The results have just been published online in Injury. So this humble little idea has led us some places and told us some things. What were those things then?
As you will note, the commercial warmer was the only method that reliably warmed the blood to something like a physiological level.
The change in temperature as the products pass through the line itself was more than we’d expected. Even the measurement of temperature just a little bit distal to the bag of blood showed a sharp step up temperature (that mean was 9.40C).
Any of the options that weren’t the commercially available device here guaranteed very cold blood reaching the end of the line. After all, 180C is the temperature we aim for when setting up deep hypothermic circulatory arrest in the operating suite. It is very cold. Should you even consider packed red blood cells if you aren’t going to warm them effectively?
In some ways, these aren’t super surprising items but small things like this can still be valuable. This was a humble little bench study of a simple question. Still, finding out that a device does what it says on the box by direct observation is reassuring. But …
We Have Questions
Research is very often an iterative process. Ask a question, provide answers to one small element of the initial puzzle, find another puzzle along the way and define a new question to explore. Each new question contributes more to the picture. On top of that, finding our way to the lab set-up and squeezing in the measurements around other work has taken a bit of time and things have moved along. This itself suggests new questions to ask.
Will everyone’s questions be the same? Well here are ours, so you tell us.
Now that we’ve come up with a lab set-up to test the manufacturer’s recommended use, what about testing a situation that more closely matches how the warming device is used at the roadside? As noted in the discussion, we don’t use machines pumping blood at a steady rate of 50 mL/min. How will a warmer perform at the much higher flow rates we demand in prehospital use? Will it still be a warmer or more of a tepid infusion system?
Are all devices the same? We didn’t choose the Buddy Lite because we were after a sweet, sweet money deal. It was the only prehospital fluid warmer with Therapeutic Goods Administration registration in Australia. There are now at least 2 other devices weighing less than 1 kg on the international market. They also advertise an ability to work at higher flow rates of up to 200 mL/min.
Are there are other potential problems when you warm the blood with these low dead space solutions? Let’s just imagine for a second you’re a red blood cell rushing through a warmer. In a pretty small area you’ll be put through a temperature change of over 200C within a system aiming to maximise that heat transfer in a very small bit of space. That implies the pressure change across the warming device could be pretty sizeable. When you get to the end of that little warming chamber having effectively passed through a very high pressure furnace, is there a chance you might feel like you’re going to disintegrate at the end of it all? What we’re alluding to is maybe, just maybe, does making red blood cells change temperature quickly while rushing through the system at up to 200 mL/min leave those red cells happy or is haemolysis a risk? If it was a risk, would the patient benefit from receiving smashed up bits of red cell?
Now that we’ve established a good model that will let us do rigorous testing,we can ask those new questions. Without the simpler first question, we wouldn’t be so ready to get going. Those new questions would seem to be how do modern devices perform at flow rates useful for the clinician rather than the marketing pamphlet? And what happens to the red cells in the process?
That’s the space to watch. Because that’s where we’re going next.
Notes and References:
Here’s the link to the prehospital massive transfusion case report mentioned near the start.
That image of the fire is from flickr’s Creative Commons area and is unaltered from the post via the account “Thomas’s Pics”.
And did you get this far? Good for you. Much respect to all those who read to the end of a thing. For this you get a reminder that you can follow along by signing up to receive updates when we post.
You also get the word of the week: colophon [kol-uh-fon] which is a publlisher’s or printer’s distinctive emblem used as an identifying device on books or other works. Alternatively it can be the inscription at the end of a book or manuscript.
Not that long ago Dr Alan Garner described the process for developing Carebundles as part of trying to deliver the best care and measure it at the same time. Here’s the first of the follow-up posts: on TBI.
The isolated severe traumatic brain injury bundle
As a follow up to our blog about Carebundles and their general utility in Prehospital and Retrieval Medicine we thought we might go through each of the bundles that we are using in Sydney and discuss our rationale for why we included the items we did and the evidence base for them. We hope this process will provide us with some open peer review of our criteria across an international cohort of our colleagues which can only be good for us.
The first thing to note is simply a repeat of my previous post. It is hard to get good evidence in the space we work in and much of the data is extrapolated forward from in-hospital practice. Mere geography alone should not affect pathophysiology so this approach is biologically plausible but we acknowledge it is not ideal. To quote from the previous post:
“We then turned to the evidence based consensus guidelines, Cochrane reviews and good quality RCTs to define the Carebundle items. This is a sobering process as you realise just how few interventions there are that have good evidence to back them up. This is particularly true for prehospital care where we are often operating in an evidence free zone. In many cases we had no choice but to go with the consensus (or best guess as I like to call it). We decided that we would include intubation for unconscious trauma patients for example despite the evidence not being all that strong and in many cases contradictory.”
So let’s look at our bundle items for isolated severe head injury (GCS <9) and why we chose them:
Intubation and mechanical ventilation
As I have already stated the evidence here is not strong. However it certainly allows better control of both oxygenation and ventilation (PaCO2) so it makes sense and is the in-hospital standard of care. We also know that we can do this safely and extremely rapidly without delaying in-hospital care (CT scan in particular). Given we are not delaying subsequent care it seems reasonable to intubate these patients on scene given the other advantages.
Again see Davis’ papers on this subject. We are wanting low normal range (in the 35-40mmHg range) but we don’t have formal blood gases available to us in our rapid response urban operation in Sydney (we do in our longer distance transports in other parts of Australia and internationally). We therefore assume there will be a small gradient from arterial to alveolar and aimed for an ETCO2 that was likely to get our arterial level in the zone we were aiming for.
Monitoring
Our minimum is ECG, SpO2, non-invasive blood pressure and waveform, quantitative ETCO2. These are the minimum standards for managing an intubated patient in our part of the world as covered by the specialty colleges. .
Venous access
There is definitely no randomised controlled trial that shows that prehospital venous access improves outcome from severe head injury (or anything else that I know of either). However it really goes with intubation as above. We aim for pharmacologically smooth intubations without desaturation or hypotension. We need a line to achieve this.
C-spine immobilisation
Note that this does not say a rigid collar, just immobilisation which can be achieved in a number of ways. There is of course evidence that collars impede venous return and therefore it is possible they have an adverse effect mediated by effects on cerebral perfusion pressure. The consensus guidelines still cite the evidence of C spine injury associated with severe head injury so neck immobilisation made our list. We’re actively reviewing what to do when we arrive at a patient already with a rigid collar in place.
Analgesia
No evidence that I am aware of that prehospital analgesia changes outcome for patients with severe TBI, even in terms of subsequent post traumatic stress disorder in survivors. Unconscious (but not completely obtunded patients) still feel and respond to pain however. Of course it may also mitigate the risk of hypertension potentially exacerbating intracranial haemorrhage so again a biologically plausible mechanism for a benefit. I think we mainly included this one as it is what we would want for ourselves & our families.
Head elevation (External Auditory Meatus above JVP)
This is again extrapolated forward from standard in-hospital care. We need to get the brain above the effect of venous pressure to maximise cerebral perfusion. No prehospital studies on outcome (recurrent theme) but seems reasonable.
SpO2 >93%
All the large observation data sets about this quote 90% as the magic number (See Randal Chestnut and Michael Fearnside’s classic papers on this topic for example). We were simply conservative and aimed a bit higher at the inflection point of the Hb dissociation curve as desaturation occurs so rapidly below this point. I note that the Germans (ADAC) are aiming for 95% presumably due to similar thinking.
Systolic Blood Pressure >110mmHg
Again the classic papers talk about 90mmHg for this item, although if you look at the Brain Trauma Foundation guidelines, they suggest a preference for a higher target, even though they can’t say exactly where to land. Guidelines out of Italy have also recommended this sort of target previously. Again this seems to make sense from a cerebral perfusion pressure point of view.
Blood sugar level
We mandate that this be documented for all patients. Our trauma population like most other parts of the developed world is becoming older and co-morbidities are increasingly common. This one is too embarrassing to miss.
Scene time <25 mins
One fifth of patients with severe head injury have a drainable haematoma. We want to maintain a sense of urgency among our teams. Again, we recognise that there are times when circumstances stop the team achieving this. The key thing is maintaining that sense that forward momentum can be significant for the patient.
Transport direct to trauma centre
All based on observational data but taking severe trauma patients direct to designated specialist trauma centres is standard of care internationally. Even the UK have got in on the act recently.
Conditional item
Hypertonic saline if neurologically deteriorating or lateralising signs
This one is going to be controversial. Again based on beneficial effects on ICP in the ICU setting rather than hard evidence of improved outcomes. We chose hypertonic saline over mannitol as there is less electrolyte disturbance and hypotension. We are targeting the neurologically deteriorating and lateralising signs group as they may have drainable lesions and we are trying to buy time to surgical evacuation. That is the theory anyway.
This is our audit sheet that the doctors complete post mission. You will note that it contains space for the team to comment on variations from the bundle so that we can identify the reasons that we are unable to meet our management targets.
Here it is in all its documentation glory.
Although the bundle is designed for patients with GCS<9 in reality we intubate a lot of head injury patients with GCS 9-12 as well for various reasons. We do not consider application of the bundle mandatory in this group but if they do intubate the patient we encourage our teams to apply all the bundle items as well as completing an audit sheet post mission.
Did we get it right? As I said the lack of good evidence makes this process very sobering, so we would particularly welcome feedback. Next time I will have a look at our blunt multiple trauma bundle.
Notes and References:
One of the papers suggesting letting CO2 rise isn’t great:
Don’t forget we’re always interested in thoughts, comments, feedback and tips.
If you like this or any of the other posts, you might like to track down the bit on this page that lets you subscribe so you can get a notification when we put something up.
Well finally we have a second podcast up. This is a quick chat about an approach to traumatic cardiac arrest, given the recent publication of guidelines we all like to read. The chat features Alan Garner and Andrew Weatherall and also touches on use of the AAJT which was recently added to the plan at CareFlight.
As always feedback, comments and insights from elsewhere would be gratefully received. If you like the podcast you could even consider leaving us a review over at the iTunes site. Or follow the site here to get a friendly e-mail when a post goes up.
Of course there are some notes to go with the podcast.
Alan mentions the HOTTT drill stuff. Here’s the package that goes with it. HOTTT Drill
There’s also a few papers worth looking at for comparison:
Dr Andrew Weatherall with an introduction to a new type of thing (well, for this site anyway).
*Ahem* [clears throat].
Well, we finally thought we should try chatting. After much delay we finally sat down and tried recording a chat with a microphone. And then after a much longer delay I have finally spent some time learning what to do with all that noise. All that slightly-too-quick-talking noise.
This effort features me chatting with Dr Alan Garner about those times you need to decompress the pleural space. It seems to be an area where a lot of people have passionate ideas about how and when to intervene. This makes it ideal for a chat, although maybe harder to be definitive about what to do. While Alan makes the argument that many of the disadvantages of tube thoracostomy first solved by the open technique have other solutions apparent in modern practice. However, all the options have some advantages and disadvantages, benefits and complications. That’s part of why it’s such an interesting topic.
This would be the point for a tenuous link to the concept of lying back and enjoying the talk like this otter. It’s just an excuse to share the otter.
I do need to share some extra bits of information, because it turns out 30 minutes of chatting still leaves some things unsaid:
This is very much a learning thing at this end. So if there’s a few rough bits in the audio/recording and the like feel free to send some constructive feedback. Promise to get better at it.
This chat actually happened way back in December (!!!) so apologies for taking this long to get it together. What that does mean is there’s a couple of bits that need an update – most particularly that the good Dr Garner has moved on from the Medical Director position at CareFlight. The excellent Dr Toby Fogg does that now (while Alan is still working pretty much as hard as ever, just not everywhere all at once).
At the end of the podcast, we have a chat about the need for research. Well I don’t know if that got him moving but Alan is now putting together a retrospective study involving lots of centres and services across Sydney. Hopefully this will provide some more evidence to add to the mix and inform how to do future research better.
Now some papers are mentioned by Dr Garner as he goes along. So,
As a bonus, here’s a reference for one looking at tube thoracostomy placement (as in whether it ends up in the right place, which was the case for 78%) which sort of highlights the importance of choosing the right bit of kit and being trained well:
Oh, and as a tracheal tube is sometimes suggested as an alternative to an intercostal catheter, it’s worth looking up this recent letter to the editor from Emergency Medicine Australasia, where a patient was unstable during transport with a tracheal tube in place to maintain the thoracostomy and subsequent investigation in hospital showed it had migrated. Yep, all techniques have their problems.
Minh Le Cong reminded me that the draft NICE guidelines relating to trauma are up for people to comment on and obviously mention chest injury amongst many other things. Well worth a look (possibly via the excellent summary by Natalie May at St Emlyn’s.
Hope you enjoy it.
Wait, there’s some more acknowledgements:
A big thanks to Dr Minh Le Cong for the encouragement and advice.
We tried out two bits of music for this podcast and they were sourced from the lovely Podington Bear at the Free Music Archive. The first is ‘Mute Groove’ off the ‘Equatorial’ album. The end track is ‘Dole it Out’ from the album ‘Grit’.
Along the way I also picked up many useful tips from Joel Werner and Samuel Webster (disclosure: the good Mr Webster is my brother-in-law but is quite a good artist and everything person and I suspect I would have come across his work anyway).
The image here was from the flickr Creative Commons area and shared by Peter Trimming. It isn’t altered.
A brief note: I get to do the editing duty this week (Dr Andrew Weatherall that is) and I could not let it pass without a word of tribute to Dr John Hinds. I had only had the chance to learn from the good Dr Hinds via his online presence. It was a big presence.
As one who did not know him personally, I can only reflect that he demonstrated many of the best qualities of a passionate doctor and that his passing, far too soon, has revealed many of the best qualities of his colleagues.
Just in case you needed another reminder, you could watch him in action here, or read good words by @Eleytherius here, or sign a really worthwhile petition to deliver a vision for a better prehospital service for patients in NI here.
As to this week’s post, Dr Alan Garner has a post on looking for the right outcomes so we’re doing the right thing for our patients.
Can’t see the wood for the damn trees
As part of their intubation quality program many services now report their first look intubation rate. We have been doing so for a couple of years now. This looks like a really good thing to do. We know that more than one attempt at intubation is associated with greater incidence of serious adverse events in critically ill patients, and the more attempts the more likely those adverse events become (reference 1).
Therefore a strategy of aiming for first look success is probably a good idea, a strategy that my own service employs. So this should be a good thing to report as a quality measure too. Indeed why would you not? After all, the more attempts, the worse things get right?
Well wait a minute …
First let’s have a think about why we would report it. Is it telling us something that actually matters?
The outcomes that really matter are did they die or end up with hypoxic brain injury. The process issues that really matter are did they get hypoxic or have a cardiac arrest during the intubation process. There are other hard complications/process issues you can measure too like aspiration with unnecessary additional ventilator days, or even did you break their teeth.
First look intubation tells us none of these things. It does not tell us if the patient became hypoxic, aspirated or even arrested. Yes it is associated with lower incidence of these complications but it does not tell you if the complication actually occurred.
And what if emphasising first look intubation rate as a quality measure shifts the focus in the wrong direction? Could you risk making the risk of hypoxia higher?
Am I losing the plot here? Let’s go back to first principles.
The outcomes that really matter are death and hypoxic injury. I don’t think anyone is going to argue these should be avoided. Fortunately the incidence of these is pretty low so we tend to use surrogates for these things instead, things like the incidence of hypoxia or hypotension/bradycardia during intubation. These are pretty direct measures reflecting outcomes that matter.
First look intubation isn’t an outcome. It’s not even a surrogate for an outcome – it’s a surrogate for a surrogate of an outcome. My concern is that surrogates for an outcome, rather than the actual outcome can lead you way up the garden path. The MAST suit again comes to mind. The patient’s BP went up so it had to be a good thing surely. Of course when someone finally did a decent study on the outcome that really mattered, mortality, it was trending to worse not better.
Although there are no randomised controlled trials showing hypoxia to be bad for you, the circumstantial evidence is pretty overwhelming so I agree this is not quite like the MAST suit situation. However in using first look intubation as a quality measure we are now reporting a surrogate for a surrogate of the outcome that actually matters. I.e. we are reporting first look as it is associated with lower rates of hypoxia because lower rates of hypoxia are associated with lower rates of death and brain injury.
This is a risky game and recent audits of my own service show why. For the past year we have had a monitor that records the vital signs every 10 seconds and we download the data at mission end and attach it to the record. I have been going through these records to see what our rates of peri-intubation hypoxia actually are.
First thing I need to say is that our first look intubation rate so far this year is 100%. However we did have a couple of episodes of significant hypoxia.
My concern is that by reporting the first look rate, we draw attention to it and we send the message to our teams that this is the thing that we think matters. So better to press on a little bit longer even though the sats are falling to make sure I nail that tube first time!
What was the big picture again? [via Jarod Carruthers on flickr under CC 2.0 and unaltered]Why are we reporting a surrogate for a surrogate? I have really accurate data from the monitor on the peri-intubation hypoxia rate, hypotension, bradycardia and arrest. Why report a surrogate for these things that might actually encourage our staff to focus on the surrogate and cause an episode of hypoxia, bradycardia, hypotension etc.
It remains important to emphasise optimising conditions for the first intubation attempt as that appears to have lower complication rates. However it is a means to an end. We should emphasise the outcomes (or at least the surrogates with only one degree of separation from that outcome) that matter. Why report a surrogate for a variable when you have the data to report the actual variable?
Some services like our own are now reporting 100% first look intubation rates, but no one is yet reporting 0% peri-intubation hypoxia rates. Aim for first look intubation as that appears to be a smart strategy, but tell your people it is the hypoxia that matters by making that the centre of attention in your reporting.
What do we mean by hypoxic?
Another thing I have been forced to look at is the definition of peri-intubation hypoxia. I had intended to use the definition of hypoxia used in many of the studies on this subject:
“Desaturation was defined as either a decrease in SpO2 to below 90% during the procedure or within the first 3 minutes after the procedure, or as a decrease of more than 10% if the original SpO2 was less than 90%.” (reference 2, see also 3-5)
I excitedly opened the data file of our first patient that we had intubated when we got our shiny new monitor a year ago to see what had happened. It was easy to identify the timing of intubation from the capnography data as we routinely pre-oxygenate our patients with a BVM device with the capnography attached. The sats pre-induction were a steady 90%, for 2 readings they were 89% (20 seconds) and then climbed to 98% when ventilation was commenced. So according to this definition we had a desaturation!
I don’t think anyone would claim a fall in SpO2 of 1% is clinically significant. It is also less than the error of the measurement quoted by the manufacturer of the oximetry system. This set of circumstances is not going to occur that often but it does not make sense to classify this case as a desaturation. We have therefore modified our definition to:
“Desaturation is defined as either a decrease in SpO2 to below 90% (minimum change at least 3%) during the procedure or within the first 3 minutes after the procedure, or as a decrease of more than 10% from the pre-intubation baseline if the original SpO2 was less than 90%.”
So what should we be reporting?
Thomas reported that each subsequent attempt at intubation was associated with an increased risk of hypoxia, aspiration, bradycardia, cardiac arrest etc. If we have the data on these variables then why not report them directly instead of reporting the surrogate for them. For hypoxia I would suggest our slightly modified definition above.
As for other variables why not use the definitions from Thomas’ paper?
Bradycardia
HR <40 if >20% decrease from baseline
Tachycardia
HR >100 if >20% increase from baseline
Hypotension
SBP <90 mm Hg (MAP <60 mm Hg) if >20% decrease from baseline
Hypertension
SBP >160 if >20% increase from baseline
Regurgitation
Gastric contents which required suction removal during laryngoscopy in a previously clear airway
Aspiration
Visualization of newly regurgitated gastric contents below glottis or suction removal of contents via the ETT
Cardiac arrest
Asystole, bradycardia, or dysrhythmia w/non-measurable MAP & CPR during or after w/in intubation (5 min)
For the physiological definitions Thomas includes percentage change from baseline like we do with the hypoxia definition. This acknowledges that these are critically ill patients and often have deranged physiology before we start. These definitions can therefore be used in the real world in which we operate. If we all adopted these definitions we could meaningfully compare ourselves with Thomas’ original paper and with each other.
And as for us…
We are seriously thinking about ditching the reporting of first look intubation rate. It is not telling us what really matters – and we can’t get better than our current 100% rate anyway. Despite this we are having occasional episodes of hypoxia and other complications, and it is possible that the rate of these complications are being exacerbated by emphasising first look.
We are therefore looking at moving to the much more comprehensive set of indicators used by Thomas (along with our modified hypoxia definition). This will demonstrate to our team members the factors that we think really matter, because we measure them and report them externally.
You could argue that the only way to achieve 0% hypoxia is to accept that we are not going to have a 100% first look intubation rate. I for one would gladly give up our 100% first look rate if in doing so we achieved 0% hypoxia. I don’t yet know if this is achievable but I have some ideas. Those who walk the quality & patient safety road with me know that we might never arrive, but that should not deter us from the journey.





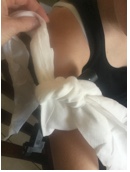



















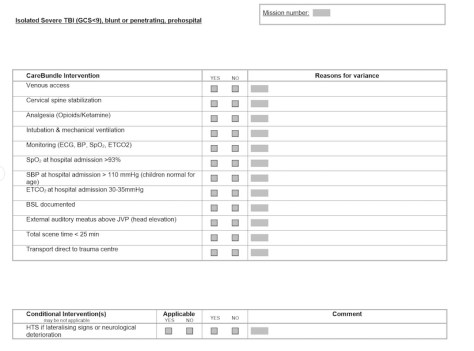

![What was the big picture again? [via Jarod Carruthers on flickr under CC 2.0 and unaltered]](https://careflightcollective.com/wp-content/uploads/2015/07/trees-copy.jpg)
