Back with another instalment in the popular series “I wish I knew then what I know now” is Greg Brown, current Education Manager / Clinical Nurse Consultant with CareFlight and former Australian Army officer.
Intravenous cannulation: the art of finding the biggest tube with a sharp point in your kit and placing it in the most proximal vein you can find so you can deliver various fluids or medications that may or may not make the patient feel better but certainly help you feel as though you have achieved something.
Okay, this might be a bit of a stretch – but in all seriousness the ability to gain and maintain dedicated vascular access in your sick patient is a vital component of medical care for nurses, paramedics and doctors alike. For many (both in and out of hospitals), the ability to find that elusive vein is a point of pride, and getting that solid red flashback in the chamber of the cannula is at times the cue for the treating team to stop holding their breath.
But the IV cannulation process is not complete once the [insert name of your service’s approved form of IV dressing] is applied. In the retrieval world, an IV cannula is almost always going to have fluids flowing through it (or at least attached to it). Having fluids attached gives the healthcare provider a ready-made flush for those medications that are used in treating the patient. Want to give a bolus of IV ketamine? You are going to need an IV flush. IV fentanyl? Flush. IV anything? Flush. You are going to be flushing everything, so you might as well attach a 1000mL bag of “flush” via a giving set and have it ready at all times.
Herein lies the problem. For anybody who has ever had to move a patient with an IV line attached, you know just how easy it is for that line to get snagged – and before you know it, your precious cannula is now no longer in a vein and instead is irrigating the helicopter floor / CT machine / footwell of the crashed car etc. Your service’s approved form of IV dressing might be awesome at holding an IV cannula in place, but it is no match for the body weight of that burly rescue technician with the IV line inadvertently wrapped around his leg who is moving in the opposite direction to the patient.
Laws to Live By
Many years ago at CareFlight, one of our “grey beards” (Dr Blair Munford, anaesthetist extraordinaire), came up with what we now call ‘Munford’s Law of Taping’ which states:
“The length of tape used on the patient should not exceed the distance between the point of injury and the receiving hospital, but anything less is acceptable.”
Taping IV lines is a good thing, but tape doesn’t work great on wet, hairy or dusty patients. Sure, you can circumferentially tape the IV line to the arm such that the tape sticks to itself and not the patient, but that is a lot of non-stretchy tape.
Story time. Many years ago, whilst on deployment with the Army, I was tasked with transferring a civilian casualty from the scene of a vehicle accident to a landing point whereupon she was to be whisked away to a United Nations hospital by helicopter. The accident involved an overcrowded minivan which failed to negotiate a corner resulting in it rolling. The knock-on effect was a mass casualty incident halfway between two forward operating bases. Medical and security assets were despatched to the scene, including myself as a young (ish) nursing officer.
After the usual initial chaos that results when medicine and tactics collide, we dutifully set about the triage and treatment of casualties in accordance with priorities and started stacking inbound AME assets. Unfortunately, given the topography, the AME teams could not land on site; therefore, we were required to ferry the casualties from the scene to a landing point about 2km away.
One particular casualty of mine was a lady with a mid-shaft femur fracture and a handful of broken ribs. I had applied a Donway Traction Splint to the leg, some oxygen and was trying to bump up her blood pressure with crystalloids whilst controlling her pain with increments of IV morphine. I had placed an IV in her antecubital fossa and had “secured” the giving set with some tape. However, despite the accumulative administration of a lot of morphine (the exact dose escapes my memory), she was still very obviously in pain. The problem? As we loaded her into the vehicle, the IV line became looped around the stretcher handle and the cannula had dislodged.
Ordinarily I’d have just placed another IV and started again; but in this case I had two problems: (1) being a mass casualty incident my stores had been pillaged leaving me unable to place another IV, and (2) the Blackhawk was already flaring (meaning it was about to land), so I didn’t have time to go back to the scene to grab more stuff. This was a major fail when it came to managing this patient. And in addition, the woman’s pain and lack of analgesia were about to become the AME team’s problem, but the embarrassment of losing the ONLY IV access this patient possessed was mine alone.
But, in the words of S.E. Hinton, “that was then, this is now”.
Simple Solutions
There exists a remarkably simple solution to this problem, and it involves a bandage. We now teach this technique to anybody who will listen because, quite simply, there is no good reason for losing an IV. It works on the side of the road; it works in an ambulance; it works in Emergency Departments; and interestingly, it works really well in those dementia patients that occupy their time by trying to undo every single medical intervention you’ve applied during your 12 hour night duty!
Step 1: Place an IV cannula in your patient in accordance the patient’s need and your ability / scope of practice. Apply whatever dressing your service says you should.
Step 2: Attach your primed IV line as per the application of common sense. Ensure that the roller clamp on the line is as close to the bag as possible – you will need to be able to access it.
Step 3: Run the IV line down the limb around 10cm / 4in and cover in a bandage (the broader the bandage, the faster the technique), leave a loop then bandage the IV line back up the limb.
Step 4: Repeat step 3 ending with the free running end of the IV line heading towards the head of the patient (this is where you will be located; if you need to replace the IV bag it’s best if the bag is close to you).
Step 5: Secure the end of the bandage with some tape. Ensure that you leave the side injection ports of the IV line accessible. You may even wish to mark these with tape so that you can find them quickly when under stress.
When you secure the IV line with these superimposed S bends you create 40cm of dead space that will take up the strain on the line if the line is pulled. Once tension is applied to the line the loops cinch together to take up the strain. More of a visual learner? Yeah, me too. See the images below.
What I now know that I wish I knew then is that performing this technique takes no longer than trying to apply copious lengths of tape to a patient’s arm, especially when that arm belongs to a sweaty, hairy person. I also know that I never again want to be the clinician whose handover includes “well, there was an IV in the arm but I kinda lost it in transit…” If it is worth doing, it’s worth securing.
Notes:
We bet this isn’t the only way to secure a line. Got tips for us to learn? Then put them in the comments. We like learning.
And remember if you like stuff on here, have a think about sharing it around. And maybe sign up to get an email when a post hits.
Respect for the classics doesn’t mean being stuck with them. Here’s a refresher on why you might not want to do RSI like they used to by Dr Andrew Weatherall. This one is a cross post picked up from the paeds anaesthesia site he chips in on, www.songsorstories.com
Everything in medicine needs the occasional reboot. I mean not as often as Hollywood thinks we need to reinvogorate a superhero franchise but at least every now and then. Sometime that’s because we learn new things (cross reference here). Sometimes it’s because our perception of what is the biggest risk changes (more on that in a second). And sometimes we suddenly realise that the original reason something became fixed practice might not have been a thing in the first place.
Which brings us to RSI, a classic so many of us have grown up with.
What is this thing?
The story of RSI starts with excellent intentions (and for this version of events I’m leaning heavily on this review by the excellent Thomas Engelhardt). In this case the idea was to come up with a safer way to get the snorkel in the all important windpipe as quickly as possible to try and minimise the risk of things that should stay nestled in the gastrointestinal tract might find their way to the lungs.
And you can understand why. Serious aspiration can, sometimes, be deadly. The first piece of the puzzle was written up by Morton and Wylie way back in 1951 who described where with the patient sitting up the anaesthetist would give intravenous barbiturate then muscle relaxant and rapidly intubate them. A rapid sequence of induction and intubation. So really it’s RSII.
8 years later a description emerged of a thiopental/relaxant/40-degree head-up tilt foot-down tilt. It wasn’t for another 2 years that cricoid pressure popped up (thanks Sellick) although interestingly it included not just a bit of pre-oxygenation but also some bag-mask ventilation prior to putting the tube in.
It was another 2 years before the other classic bit of RSII became popular, with an exhortation to avoid bag-masking because of the perceived risk for gastric insufflation and hence regurgitation.
A classic technique derived from a series of “what abouts” and “I reckons”. I mean, you wouldn’t read about it. Except you just did.
That’s not to say that medicine doesn’t have space for a bit of logical derivation of good ways forward. It might just suggest that the whole approach is open to a refresh.
Re-evaluating the Likely
If the technique was designed to prevent aspiration, maybe we should start with looking at how likely this event is in a setting a bit more modern than 1951. In 1999 the epic writing team of Warner, Warner, Warner, Warner and Warner looked at 56138 patients under 18 having procedures (elective or emergency) over 12 years to see just how big this problem was. This covered 63180 procedures.
The time frame for defining aspiration was entry into the operating room until 2 hours post-anaesthetic. To score the label there had to be direct identification of bilious secretions or particulate matter in the tracheobronchial tree or new X-ray findings after an episode of regurgitation. A total of 24 patients met the criteria.
11 of those were emergency cases so the rate in that group was 1 in 373 compared to 1 in 4544 in the elective cases. 21 of the 24 were around induction. 15 of the 24 had no symptoms develop despite the aspiration. 5 of the other 9 did need respiratory support of some kind and 3 of them needed ventilation for more than 48 hours. Well the paper says that but actually describes ventilation for 18 days, 14 days and 33 days in those cases.
And there’s the rub. It’s really very impressively rare. But then when it goes bad, the downside can be very, very down.
So fine, let’s prevent the bad thing. We’d better get on with the classic old RSII, right?
Remembering the Even More Likely
The problem with being so rigorously focussed on avoiding pulmonary aspiration that you do things like not help the patient breathe, is there are other basic functions that don’t get looked after so well. Like oxygenating.
Gencorelli et al looked at episodes of desaturation during RSI while describing the classic drugs/cricoid/no ventilation technique. Across 1070 children included they reported a 3.6% rate of desaturation to 89% or below (1.7% of the patients being in the under 80% group). Not surprisingly the under 2s were more likely to have a desaturation.
These rates are low of course and certainly lower than in some other areas of practice. Reports from emergency departments have indicated desaturation rates anywhere from 14% to 33% (with the latter reporting rates of desaturation of up to 59% in the under 2s).
So amongst the various things we’re trying to do to prevent the 1 in 400+ event are we at risk of failing on another key thing. You know? The oxygen provision thing.
What’s the alternative?
Neuhaus and team subsequently described very well their approach to RSII, which they badged as cRSII (where the “c” is for “controlled” not some other “c” word like “cheese” which wouldn’t make sense anyway but would be a good reminder that cheese is great).
They key features for them (putting to the side “lots of preparation”):
20 degrees of head up (though they say only for the over 2s)
Suction any NG in situ.
Give the drugs.
Avoid cricoid pressure (with a few exceptions).
Provide gentle facemark ventilation with peak pressures of 12cmH2O.
Neuromuscular monitoring to ensure the muscle relaxant has really, really worked.
This last point makes a heap of sense as active regurgitation is a problem created by airway instrumentation when you don’t have adequate anaesthesia and paralysis.
It’s a big list.
Talk is cheap though, what were their results?
They report on 1001 patients They had a moderate hypoxaemia (89-80%) rate of 0.5% and a severe hypoxaemia (< 80%) rate of 0.3% and the 8 patients this represents had a median age of 0.8 years. They had 1 patient with regurgitation but no evidence of aspiration.
That’s pretty impressive.
Putting it Together
So if we accept that we should really try and optimise oxygenation, and that the risk of this is higher than the risk of aspiration then we have to accept that modifications to that original technique are reasonable. What are a few steps for practically putting it together?
1. Assess that risk of a full stomach
It might well be that we’re going to avoid cricoid most times, but there are still a few situations where that risk of aspiration is probably higher. In the Neuhaus paper they suggested achalasia, Zenker diverticulum or post-colonic interposition patients (done for oesophageal replacement) always need cricoid.
It certainly seems worth having heightened concerns in the patient with significant increases in intra-abdominal pressure.
2. Everyone sits up
Why wouldn’t you have a bit of head up? It makes sense if you’re avoiding passive regurgitation and is a good position for pre-oxygenation, facemark ventilation and intubation. I’m not quite sure why some authors have suggested the under 2s shouldn’t be head up. This is a routine option.
3. Have that suction handy
Goes without saying maybe, but I’m saying it.
4. Pre-oxygenation, but not with distress
Yes you want to pre-oxygenate. And most times you can talk kids through that and get a full 3 minutes in. Some kids will only get more distressed with oxygenation though, and insisting on pre-oxygenation only guarantees distress. Given that you’re going to apply gentle face-mask ventilation, it’s rare you need to go to the wall on this one.
And while I’m there what about apnoeic oxygenation? Well, as discussed in this post, the evidence that’s available in kids isn’t so persuasive as to suggest it should be routine. The stuff that has been done showing extended apnoeic time actually followed effective pre-oxygenation with face-mask ventilation. So as we’re going to put that tube in quickly after the same sort of effective face-mask ventilation, extending apnoeic time for minutes seems not that clinically relevant.
5. Cricoid yes or cricoid no?
Again this is a judgment call. I know plenty of anaesthetists who still prefer to start with it but with a low threshold to remove it. I’m more likely to mostly err on the side of not using it, except for those high risk of aspiration patients.
If you are going to use it, it is worth noting that, particularly in infants, the trachea is quite often more prone to distortion by cricoid pressure than you realise. Doing flexible bronchoscopy work you’re sometimes asked to manipulate the airway and I’ve seen the whole trachea get substantially compressed and distorted by seemingly innocuous manipulation. Distort it enough and you can increase the resistance to air going in and out enough to make it easier to get down to that stomach.
In addition, as covered very nicely in this review, cricoid relies on the alignment of trachea and oesophagus and the evidence is that in kids < 8 years old 45% had displacement of the oesophagus so you’d be unlikely to get compression of the oesophagus even with perfectly delivered cricoid (at least on the CT scanning mentioned).
So for the very high risk ones I’d tend to start with it (well start with it once I’m sure the kids won’t react to it going on), but that leaves almost everyone where I would’t be too concerned. And if it is on, I’d be quick to take it off if it was impeding either view or tube passage.
Maybe I included this picture of an echidna because they have a reputation for being good at waiting and not because it’s a prickly situation.
6. Wait
We’re going to take our time with face-mask ventilation and maintain oxygenation. So where’s the extreme rush getting the tube in? Being too obsessed with that step, even though you’re achieving oxygenation, is a way to end up instrumenting the airway while the patient is only lightly anaesthetised or inadequately provided with paralysis. What was that thing we’re preventing again? The regurgitation thing that’s worse if we get going while the kid is lightly anaesthetised? Oh, right. Slow down.
The description suggests using a nerve monitor. I can’t say this is routine myself, but once the muscle relaxant is onboard I do publicly note for the team I’m working with how long we’ll be waiting on the clock before we start trying to intubate. (“The clock says 09:30 now. Once it ticks over to 09:32, we’ll start with the intubation.”)
I then remind everyone that this will take an unnervingly boring period of time and they might want to come up with a good joke to fill the time.
7. Ventilating
Yes, this is a thing that’s necessary because kids desaturate quickly. Particularly the younger ones. Achieving gentle face-mask ventilation relies on really good technique with the bag in hand. Plus it’s very therapeutic to gently squeeze that bag.
7. What about parents?
This one also needs an assessment of what might help and what won’t. For lower risk kids, as a paediatric anaesthetist doing it regularly, I’d be comfortable having them along. But if it was the sort of case that was likely to be difficult, or if I was back at the training junior doctor stage, there’d be no dilemma for me. I’d tell the parents that they wouldn’t be coming in. Having them alone to help their child relax (not always a guaranteed result of having parents in) has some advantages. But the prime job is safe management of the peri-induction period. And that might mean less people around.
So those are the simple things that have shifted over the course of my time in the big wide medical world. It’s a realignment of the priorities in a way that makes the ‘R’ in ‘RSII’ look smaller and smaller so that the oxygenation is placed at the top of the tree.
Put together though it’s a reboot worth endorsing. I mean the 60s just weren’t that great, surely?
Notes:
How many bits that are really important aren’t covered here? There must be some. So leave a comment. We’ll all learn.
And if you like the post and other things around the joint, maybe throw your email in the relevant spot so you’ll get an email each time a new post pops up.
This post is a cross-post from another site that this Weatherall bloke works on called Songs or Stories. It’s about paediatric anaesthesia.
That echidna pic came from flickr’s Creative Commons area and is unchanged from Duncan McCaskills’s post.
Now to the literature, because going to the direct papers is always rewarding.
That review by Engelhardt where he makes it clear what he thinks is this one:
It seems like a simple thing that’s a given – delivery of good analgesia. Except for the bit where good clinicians fail over and over at this. Here’s Dr Alan Garner checking out a recent study from the Swiss that looks at some of the holes.
As prehospital clinicians I think we all aim to provide as technically sound and evidence-based management as we can. This is a given but when I think about what I would like for my own family or myself I also want “care”. This is what makes health care interactions more than just an exchange of services for money. And this is what sends me crazy when I hear patients described as “clients”.
But I am digressing. A major component of care is the relief of suffering and the most common form of suffering we see in the prehospital world is pain. Good pain relief early might not change the patient’s probability of death in the longer term but it might well change functional outcomes such as symptoms of post traumatic stress disorder. But most of all we should do it, and do it well because we care.
There have been a lot of studies published about management of pain in emergency departments and it almost always looks bad. People with obviously painful conditions either not getting analgesia, getting it late or not getting enough. Given that the most common single presenting complaint to emergency departments is pain of some kind, I would argue that a fundamental KPI of good emergency care should be time to adequate pain relief and this should be reported above the 4 hour rule, access block and any other process indicator. Waiting for a bed for hours is regrettable but waiting for hours in agony is simply barbaric.
If EDs are doing it badly you can be reasonably confident that prehospital is worse given all the additional constraints. A new study has just been published by the guys from REGA (Swiss Air Ambulance) building on some work they have done previously around the prehospital analgesia question. The work arose from a quality assurance project on analgesia that they have been conducting across their organisation to try and improve pain management and they are much to be commended for sharing their work on this. They have allowed us a view into their struggle so we can learn from them.
And it has been a struggle. In this new study they documented that one in six patients with moderate to severe pain (defined as >3 on a 0-10 numerical rating scale as reported by the patient) did not get any prehospital analgesia at all! This is even more noteworthy given that the physician documented the pain score of >3 at the scene but apparently did not act on it for some reason. One clue might be that a predictor of inadequate analgesia was shorter scene times and more severe injury (higher NACA score). I was wondering if hypotension therefore might be one of the drivers for no analgesia but “circulation insufficient” was pretty uncommon being present in only 13 of the 778 conscious patients in this study (this stuff is in Table 1 in the paper).
Local Stories
Several years ago we audited the analgesia given to children by our own service. In some cases we did not give analgesia for clearly painful injuries (like bent long bones) but there was evidence that the road paramedics who had been there ahead of us had done so. There is no mention of this occurring in the Swiss study. Perhaps this might partially explain the lack of analgesia given if this is also occurring in their system. Although even if this did occur the physicians still documented pain scores >3 whilst the patient was in their care which you would have thought would prompt further analgesia.
I am not meaning to be too critical here. In the audit of our own service that I mentioned we also found cases with clearly painful injuries and no record of analgesia given by road paramedics or our doctors. This prompted a major rethink for us in our approach to analgesia in the field including formally recording pain scores on our observations chart to prompt our teams to keep this front of mind. Analgesia is also included as an item in all our Carebundles for traumatic conditions, and for intubated patients regardless of the underlying pathology. One of the risks for inadequate analgesia identified in this new study was that the patient had a non-trauma problem. It might be timely for us to review our Carebundles for non-trauma conditions too.
Digging Deeper
Another risk factor for inadequate analgesia was severe pain from the outset (score 8 or more). In this situation it seemed a single agent just was not enough. Judicious use of small amounts of ketamine in addition to the opioid appeared really useful here. And it appeared the combination was better in severe pain rather than just ketamine as a single agent.
I am also a little surprised about the narrow modes of delivery utilised with all analgesia given IV. In our system the nasal route for fentanyl is used frequently particularly for children and it works a treat. I also think that regional blocks have a place, particularly where the injury mechanism and your exam indicate that the injury is confined to a limb and the situation is not time critical (the time it takes is probably the major contraindication prehospital).
We have recently formally introduced fascia iliaca blocks to our service. There are lots of other blocks you can utilise , particularly if your service carries an ultrasound machine with an appropriate probe for nerve localisation. This is a skill you are unlikely to learn prehospital (except perhaps for femoral or fascia iliaca blocks) as you will never do enough of the other types to develop any skill. If part of your practice is in the hospital context where you can get lots of practice however, these are well worth learning. Done well they can completely remove the need for parenteral opiates. The context that we have used regional blocks (other than femoral or fascia iliaca) is in limbs trapped in machinery. Not a common circumstance but a useful tool to have in the box when it occurs.
The Other Bits We Rarely Look At…
I don’t think this was the aim of this study but it would also have been nice to see some attention paid to non-pharmacological methods of pain management. Good splinting and packaging is the obvious first line for prehospital services and is one of the basics that is worth doing well. We don’t carry hot or cold packs in our service due to the weight, but they are available from our local ground ambulances. These can also help in the right patient.
Plus a Slightly Unexpected Elephant
And lastly they claim a slightly unexpected elephant is in the room. Treatment by a female physician is reported as being associated with a higher likelihood of arriving at hospital with inadequate analgesia. To be honest I’m not quite sure what made them look at the gender of the practitioner but there it is, written up. Before anyone assumes this was some situation induced by most of the patients being middle-aged blokes, it wasn’t about the patient gender at all.
An actual elephant not in a room as opposed to the elephant in the study that is probably not an elephant.
So what is going on? I can’t quite figure out why this would be the case although the Swiss group has documented this previously in their own system. Is this a Swiss peculiarity or is it more wide spread?
Well to me it looks like there are a few holes in the information provided that make me wonder if it’s a blip rather than an actual pachyderm. For example non-trauma patients were more likely to arrive at hospital with insufficient analgesia than trauma patients. I can’t construct what proportion of those patients got a physician of a particular gender by chance from this report though. Could it be that the real issue is that clinicians interpret the significance of pain differently based on the context or mechanism? If it’s “medical” pain rather than traumatic pain do we tend to wait for the medicine to fix the medical, rather than treating pain separately? There’s at least one confounder for you without even trying so I’m not convinced a strong case is made that provider gender is a crucial determinant of analgesia efficacy.
A question the physician gender stat does raise that is beyond the scope of this study is the need to consider the particularities of the provider in the mix. Beyond breaking things into much larger groups (like physician vs paramedic) I don’t recall seeing much on what characteristics of a clinician make them more or less likely to provide the good juice. If we don’t understand biases that might be in play I’m not sure we can do the most effective job of changing practice.
The bottom line – be obsessed with good analgesia. It’s easy to get obsessed with all those interventions we think of as advanced, but the long-term quality of life of patients will probably be equally influenced by getting this bit right. Use a multimodal approach rather than just the parenteral one. Combine agents if severe pain requires it. Consider local and regional blocks if you have the skill.
And if anyone can figure out if the physician gender difference in this study is a blip or a real thing of some other sort hidden somewhere in the unreported elements, I’d like to know. It’d be good to show that elephant the door.
Notes:
Yes. That’s a real elephant and the photo is via @AndyDW_
There are plenty of times in the land of retrieval (and in some prehospital settings) where you need a little bit more than the simple squeezy cuff gives you. An arterial line. Maybe we could share some tips that work for at least one person with the hope of encouraging people to share theirs. This post is from Dr Andrew Weatherall.
There are things in medicine that are more than a bit disconcerting. Clinical practice pretty regularly asks us to skate back and forth between degrees of uncertainty and deal with it. So you take your reassurance where you can and sometimes that is in the form of a red wiggly line – the arterial pressure waveform. Yes, I’m that sad.
Look, here is the very evocative image that flickr threw my way when I searched for “red line” under Creative Commons. Think about it.
Given the problems associated with other monitoring methodologies in retrieval medicine having a more accurate option for providing haemodynamic information is invaluable. Add in the option for easy blood sampling and moving a critically ill patient is clearly made a lot more appealing with an arterial cannula in place than without it.
They can be a bit of a bugger to get in sometimes though. Particularly in the area I spend most of my time which is paediatric anaesthesia. Now I don’t have a bazillion answers as to how to make it sure it always hits the spot but there are a bunch of things I always do to try and increase my chances of success. Now these might be things for deploying in little people but lets face it, adults are just big kids. Pathetic, large, disintegrating kids. Anyway, in no particular order here’s a few:
1. Check them all
It’s pretty rare that you need to specifically place an arterial line in one chosen artery for prehospital or retrieval work. Not all pulses were created equal though so it’s worth taking a moment to feel all the candidates to measure them up. Choose the best one for that first shot.
2. Get the position right
Whichever one you choose, it’s worth getting the position at its best for that particular artery. At the wrist I think a lot of us have been shown the wrist extended position, and that is usually pretty useful. It’s worth exploring how extended you need that position though. Sometimes when you go to extreme you can distinctly feel the pulse get a little harder to feel. And while a roll under the hips can make a femoral line just that bit easier, it’s worth doing a before and after check. . The bigger point is that you don’t want to just choose the best pulse, choose the best position for that pulse.
3. Know your kit
This is sort of a good rule for lots of prehospital and retrieval work. You need to know your kit and choose it well. Or if you’re utilising something at the place you’re picking up the patient, make sure you understand it. Different cannulae meet up to to the needle component differently. If you’re planning to have a wire as a back-up to get in (assuming it’s not an inbuilt option) you might want to double check the wire will get through the cannula. Know what you’re wielding. Plus at the same time it’s worth remembering that a smaller cannula in the artery is a lot better than a bigger one you can’t feed in. Choose the cannula you’re sure will get in.
This also came up when I searched for “red line”. Bit of a fail there. That’s not a red line, it’s a line of red dots. It’s even called “Red Dots”. What gives flickr?
4. The Wire Bit
While I’m there, a wire can obviously be a pretty good friend. I know plenty of people who prefer the technique where you transfix the artery, come back and feed the wire up once the blood is flowing back freely. Plus get a smaller cannula in (see above) and that wire becomes the tool to dilate up to a larger bore cannula.
5. Sit Down
I know this seems really minor and maybe you feel strongly that you’re only doing it right if you’re in a moving vehicle and the family cat you brought with you to comfort the owner is sinking its claws into the back of your neck or up your nostril or something. The thing is trying to not let the environment control you is part of the gig. When you sit down you can set up your ergonomics a whole lot better and position yourself to take away muscular strain and fatigue while you’re doing it. So if the space allows it, sit down and get comfortable.
6. Side to Side and Up and Down
Now that you’ve hopefully found a comfortable position, it’s worth really mapping out that artery. Maybe other people have more sensitive fingers than me but I generally find that placing a single finger on the pulse and trying to centre it in the middle of the pad of my fingertip helps me get a sense of where it is. I then use that same finger to feel up and down the artery and figure out its course so I can mark it on the skin. It actually doesn’t matter a huge amount if the mark is perfect as long as I can go back, feel and understand where I’m feeling the artery in relation to the obvious mark I’ve made. I do this every time to help construct a picture in my head of how it all lies, even before I get onto ….
7. Use an ultrasound
If it’s available, then probably just use it. The evidence says that you’re more likely to get it in without incident and it’s unlikely to be a slower endeavour. Using the ultrasound well still demands good patient and clinician positioning as well as a scout scan up and down the artery to understand its course and any surrounding stuff. Small ultrasounds are now good enough that you should be able to pick up the tip of the cannula all the way into the middle of the vessel (and spot when you’ve still got a little bit of tissue indenting at the wall). Just use it.
8. Short, sharp, flat
It makes pretty obvious sense to approach without too steep an angle (though sometimes you can pop through the skin better with that sort of angle). A flatter approach maximises your path in the vessel which maximises your chances of staying in there. When it comes to movements I find an approach with short, sharp advances more successful than a slow steady push. At least in kids sometimes the latter seems to allow that artery to squeeze out of the way (but I’m happy to be pulled up on that one).
9. Also use local
If the patient is awake of course. Why? I think that’s actually an obvious one.
This one, also came up on the “red line” search but really it’s about the dog. So maybe if you want to get arterial lines in, think more about puppies?
10. Be ready for success
You’re probably going to be brilliant so be ready for that not surprised. Having those tapes and connections ready so you can focus on the bit after the cannula (particularly trying to maintain a clean and dry field so everything sticks and you don’t have a bunch of stuff to clean up) lets you get on with actually using the monitor.
So there is my meagre collection of practical bits and pieces. In the prehospital and retrieval space I can’t always guarantee that I can set myself up like I can in an operating theatre. When I make the effort though it turns out I usually don’t have to compromise that much. And that effort usually makes the whole thing go a little bit smoother.
It’s also not an exhaustive list. So if you’ve got a top tip then hit up that comments section. I could use a tip to be better next time I’ve got to step up to the red line.
Notes:
The main reference to read for this one would be this Cochrane review looking at success rates for arterial cannulation in kids using ultrasound. The short version is yes, do that.
All the images here were from Creative Commons posts on flickr.com. The first is from XoMEoX, the second is from Håkan Dahlström and the third is from Marco Galasso.
This is a popular series and it’s not hard to see why. Greg Brown drops back in to talk about the airway device that is now his go to item.
I clearly remember a time when the escalation of airway management in prehospital care resembled the fabled Underpants Gnomes from South Park and their three step plan to making a profit.
Back then, airway management looked something like this (and yes there were four steps, not three like in South Park):
Patient’s own airway – bummer; that’s no fun for anyone.
Oropharyngeal airway (aka the Guedel) – fun but not that inspiring.
Endotracheal tube – break out the high fives, it’s a good day to be a medic.
Needle cricothyroidotomy – if an ETT doesn’t do it, a 14 gauge cannula in the throat ought to fix it. Then there are the mutual backslaps.
Back in the day when I was new to military prehospital care (and at a time where not much was happening in the world) the focus seemed to be on big ticket items and not the purpose of the interventions. Indeed, it seemed to me that the drug of choice for any airway problem was plastic; and the bigger the problem, the smaller the dose.
What I know now is that the one’s choice of procedure must consider a whole lot more than just self-gratification. Airway problems are generally either an oxygenation or a ventilation issue, and the choice of procedure must take at least this into account. However, the purpose of this post on the Collective is not to discuss the differences between CICV and CICO (nor the relative advantages of DL vs VL) but simply to discuss basic airways.
Simple Is As Simple Does
There is no doubt that a patent airway that was issued to the patient at birth is best for the patient. Therefore, it goes without saying that anything that can be done by the treating professional to maintain a patent natural airway should be at least considered. I am not going to go into how best to clear an airway and position a patient as there are a myriad of reputable sources out there for you to conduct your own research but I will make two important points:
In a perfect world the “ideal” position will align (and therefore open) the upper airway; seemingly minor changes in positioning can have significant detrimental impacts on airway potency (and vice versa); and,
If you don’t know how to position a patient or provide manoeuvres then you might want to consider taking a step back and booking into a first aid course. Quite quickly. Like right this second. Just do it ….
Still here? Good then, on with the show.
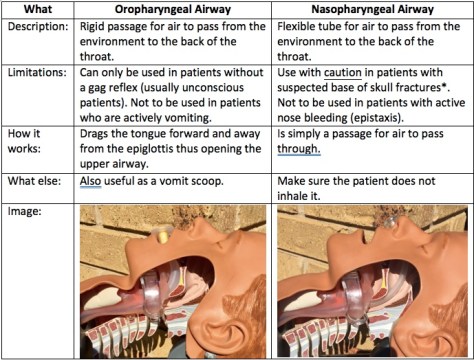
Which means it’s time to introduce one of the heroes: a simple artificial airway. To Guedel or not to Guedel? For many years that has been the question, and the oropharyngeal airway (OPA) was definitely my plastic of choice. Simple to insert and effective – two of my favourite things in a medical device. But are they deserving of their historical gold medal for simple airway adjuncts? Well, maybe yes and maybe no.
You see when it comes to simple adjuncts I have become, over the years, a massive fan of the nasopharyngeal airway (NPA). I would argue that they are just as simple to use as their orally inserted cousins – the operator just needs to be trained in their use. And whilst there are pros and cons to all medical interventions in my mind the NPA has one big benefit over the OPA – when (if) the patient starts to rouse the NPA can stay in, a handy thing for those pesky patients whose level of consciousness ebbs and flows.
Over the last ten years the NPA has gained popularity amongst first responders with thanks to support from some international heavy hitters, and not before time. You see, the NPA was actually invented before the OPA – 38 years earlier, in fact, by Joseph Clover of the Royal College of Surgeons (he later became a founding member of the Royal College of Anaesthetists) in 1870. The first OPA was designed by…. wait for it… Frederic Hewitt in 1908. The first “Guedel” was not even invented by Arthur Guedel whose name is now synonymous with the device. He didn’t enter the scene until the 1930’s (but I will grant that he made huge improvements to Hewitt’s rudimentary designs).
However, it was not until 2002 and the widespread introduction of Tactical Combat Casualty Care (TCCC) in militaries worldwide that the NPA started gaining favour once more. With thanks to a push from the United States Department of Defense’s Special Operations Command, NPA’s started making their way into the individual first aid kits of soldiers, sailors and airmen employed in combat operations. Indeed, by 2008 every Australian serviceperson employed in combat roles carried an NPA in a pouch alongside appropriate haemorrhage control devices. NPA’s are now taught as part of C-TECC guidelines (the civilian version of TCCC) and are now commonly the first artificial airway device reached for by those employed in first responder roles worldwide.
Are there risks associated with the of an NPA? Well, this is medicine, isn’t it? Of course there are risks. The big one that everybody immediately jumps to is in the patient with suspected basal skull fracture (or a fracture of the cranial vault). The risk in inserting an NPA here is that the tube may indeed enter the cranial cavity instead of heading into the nasopharynx. But a review of the literature reveals only two cases where this occurred thus making it a rather extreme reason to be afraid of using an NPA. (Note: that same review of the literature also revealed an article advocating the use of nasopharyngeal airways in the treatment of watery diarrhoea…. Four words: single use only please!)
Putting It To Work
So how do you utilise an NPA (and I’m talking about as an airway device, not in treating diarrhoea of any consistency)? Well firstly, size matters. I am sure that at some point you, like me, have taught various methods. The first common method is to look at the diameter of the patient’s pinky finger – in theory, this is the same diameter of the nares (nasal openings). Therefore the NPA of choice should be the diameter of the patient’s pinky. Yes?
Alternately, the second common method of sizing pertains to length – in theory the distance from the nostril of choice to the tragus (that flap at the front of the ear where it meets the cheek) is the same as from the tip of the nose to the upper pharynx. Yes?
Well, research by Roberts et al in the EMJ found that a combination of the two methods is required to get reach NPA nirvana and that in fact the patient’s height was a better determinant of requisite NPA size. They used data from MRI scans to determine that, all things considered, the law averages reigned supreme. Average height male? Size 7.0mm Portex NPA. Average sized female? Size 6.0mm NPA. Or, you could await the rollout of the MRI App on your smartphone of choice…
Once you have selected the correct size NPA you simply pick the largest nostril, lubricate the outside of the NPA (the patient’s saliva is usually sufficient) and insert whilst aiming for the patient’s ear (the same side as the nostril you are using). By aiming for the ear you are pushing backwards, not upwards, thus reducing the risk of the NPA entering the cranial vault in that patient with a suspected basal skill fracture. For this reason the presence of a suspected basal skull fracture has relegated to the status of relative contraindication (no longer an absolute contraindication). If any significant resistance to insertion is felt then the attempt should be aborted and the other nostril attempted.
Be sure to consider how you will secure the NPA. Certain members of society have naturally wider nares and I’ve seen them inhale their NPA. Placing a large safety pin through the shaft of NPA just below the flange decreases the chances of this happening, but in most patients I’ve treated the safety pin has not been necessary.
So there you have it – another thing that I know now that I wish I knew then is that the NPA is not an evil device guaranteed to lead any patient who has ever experienced a blow to the head on a one way trip to the morgue. Rather, the NPA is now my simple airway of choice, an intervention that I have used countless times both on battlefields and in emergency departments, and is the only airway device that I carry on every single job. Oh, and it also has some purpose in treating patients with watery diarrhoea…apparently.
Notes:
Remember if you like things on this site there’s a box somewhere where you can throw your email address so you get a regular email when a new post hits.
Want to know about how your choices of airway adjuncts can affect ventilation? Then go here.
Interested in reading more about the facts and myths of NPA’s? Try this.
Here’s a cool little video about airway manoeuvres and simple adjuncts from that good crew at Life in the Fast Lane.
And a previous post that included the use of NPA’s in the tactical environment can be found here.
This post is based on a talk prepared by Dr Andrew Weatherall for the South African Society of Anesthesiologists Congress for 2017 held in Johannesburg. As invited faculty
I think when they first offered this the plan was to do sedation in the dental chair. Which I’ve never done. And this is for a refresher course.
So we changed the topic to sedating kids in strange places. Which I have done.
But they’re strange places so by definition they should seem weird to you which means you probably haven’t done it before in which case it’s not a refresher course topic at all. Just like it’s hard to have a refresher course on swimming with sharks in bathtubs, it’s hard to have a refresher course on undertaking sedation in places people don’t do sedation.
So I guess I’ve screwed this up every which way.
Nothing for it but to sedate someone though. So let’s start with a 18 month old who has a hand injury. We’re going to sedate him to get things fixed up rather than waiting for a free operating theatre.
At the start of any sedation we need to ask some questions of ourselves. And I like to start with the Cluedo questions. The ones about “Who?” or “Where?” or “How” that help us make the choices to get this sedation done.
What are we talking about?
It’s pretty vital up front to understand what we’re describing. We need to understand what we mean when we talk about sedation.
Well as good a place as any to start is with the ANZCA documents on this (this is my low rent version of international colour for this one). ANZCA include a couple of key points:
There is an implication that you’ll be using pharmacological support to improve tolerance of uncomfortable or painful procedures.
They try and separate out some levels of sedation.
That latter one can be a little problematic but they do talk about conscious sedation, where the individual will produce a purposeful response with minimal stimulation, and deep sedation where there will only be that purposeful response with painful stimulation.
To be just this side of general anaesthesia however you do need to have some sort of response. Plus you need to consider if what you’re really talking about is analgo-sedation because you’re expecting some pain to be dished about.
Who?
The “Who?” is important in planning for a bunch of reasons. Is it you or someone else actually delivering the sedation? What’s their level of experience or expertise? What’s their clinical background? The background of the practitioner is highly likely to influence the choices they make, particularly when it comes to pharmacology.
The “Who?” also covers the patient at question because the needs of an 18 month old are not the same as those of a 12 year old, and aren’t the same as the needs of a 40 year old.
Lastly, the “Who?” question applies to the proceduralist. If you’re giving sedation to get a job done, then the needs of the proceduralist to get things done have to be taken into account.
Where?
Well, we’re talking about strange places, right? So that definitely matters for this scenario, but it matters for every sedation scenario. It will influence what you feel comfortable offering, and what help is available. It will also heavily influence where they get looked after when it’s done and might influence how quickly you want them back to their entirely normal state.
Wait, this is the strange places post so I should probably mention something….
Today’s patient is in a bathtub. He’s had his hand stuck down the drain for 2 hours with people trying to get it out. It’s 22:00. It’s about 6 degrees Celsius outside. Your proceduralist is the rescue volunteer with the jackhammer who is going to have to work through concrete to reach the bath and dismantle it.
Ready then?
When?
Well I think in this case we already know that. For other sedations though it’s worth making an assessment of when it has to be done? Does it really have to be now or can it wait a little if you have concerns with sedation. Will the timing matter for available care afterwards?
What about that fasting question? All if it helps at all there is very limited evidence that fasting intervals influence things like aspiration rate. The Pediatric Sedation Research Consortium looked at 139142 patient records in 2016. They found a total of 10 aspirations and 75 major complications. 8 of the aspirations were in kids fully fasted (though that was from 82546 records whereas the non-fasted made up 25401 cases with details). Both rates were < 1 in 10000.
Another look at 12 years of nitrous oxide procedural sedation in kids not necessarily fasted revealed 1058 cases with 0 major complications (and I think quite astonishingly only 11 cases of nausea and vomiting).
So I probably would still make an effort to fast most times, I’d also be pretty relaxed if clinical need indicated we were in a “right now thanks” scenario.
Why?
This isn’t a moment for an existential pause. It’s the key question about our goals of this sedation. Personally I find it useful to think about the ins and outs of it.
What are the sensory inputs we’re going to inflict on the patient and what is the level of cerebral output we’re aiming to see?
In radiology you might just need a little stillness. The inputs might be almost nothing, or just a little noise. That’s clearly different to a burns dressing, or a quick pull on a fracture.
Remember our little punter? This kid is stressed after 2 hours of messing about and there are 10 weird people in bright orange in the bathroom with him. They’re using noisy tools. His hand is sore. He is way past his bed time. The extrication is thought to be a 2 hour job.
Our goals are to achieve a comfortable light snooze that might have to deal with variable pain input.
How?
Finally we get to it. And you might figure we’ll dive straight into drugs. Nope. This is a super short chat so I’m more interested in an approach that will work, while assuming that clever people checking this out have an armamentarium of things they are good with.
So I think when we get to the “how?” it’s easiest to remember we need to offer some REST.
That’s
Rapport
Environment
Safety
Therapy.
Let’s work through them.
1. Rapport
In most sedations establishing a good rapport with the patient is vital. Sedation isn’t like general anaesthesia and there is the potential for recall and moments of discomfort. Establishing trust is therefore a big help, because if there is one of those moments it’s a lot more ideal if the relationship you’ve established means they’ll trust you when you try to provide reassurance. The same goes for if you’ve got a carer around.
So there are plenty of ways to work on that beyond this scope, but slowing down to take this step pays off.
Look I wouldn’t try this approach personally, but whatever works for you…
2. Environment
As much as possible setting up an environment to support the sedation is ideal. Simple things like choosing a specific spot where you can, reducing noise in the area (bugger, jackhammer), ensuring easy access to the patient and controlling the numbers of people in the space can make it a much calmer experience all round. If the environment is good, really you should need less pharmacology. The environment is also a key element of …
3. Safety
Sedation is actually pretty safe overall. Biber et al have published stats showing a 4.8% adverse event rate in 12030 patients. For the really concerning ones they only observed airway obstruction in 1% of those sedations and laryngospasm in 0.6%. 1.2% of patients needed some bag-mask ventilation. Unsurprisingly issues were highest in the 0-5 age range.
Obviously we need to be actively focussed on safety though. And I’d start with your eyes, ears and hands. Personally I think delivering good sedation can be much more taxing than giving a general anaesthetic. To keep them consistently at a state of sedation, which can be a lot more dynamic than anaesthesia, requires a continuing close quarters assessment of where they are right now and what the inputs are about to be.
So being able to reach out and touch or gently stimulate the patient matters. Close observation of respiratory patterns matter. This doesn’t suggest we should abandon monitoring. We should have at a minimum pulse oximetry, a means of measuring pulse rate and BP and I’d argue that in hospital or static settings capnography is a must.
Every sedation also requires a plan for how to manage airway complications, support breathing well and manage any circulatory issues, rare as they all might be.
Safety requires a team too. The ANZCA documents suggest that beyond yourself you need at least one person available to assist you at the drop of a hat. Or a clatter of the safety helmet I guess.
Which brings me to the last point, don’t forget PPE. That’s not just for you either. Your patient might need it.
4. Therapy
We finally got there. This really comes down to two big groups:
Non-pharmacological, which should absolutely not be considered as a lesser item. If you have some good distraction and redirection techniques they can get you a long way there.
Pharmacological.
When it comes to agents this isn’t really the space to argue for one over the other. I would say that if you’re sedating in a new spot or new situation, I wouldn’t try out that cool drug someone told you about for the first time.
Each agent has its pros and cons. Propofol is great for sedation when used right but can sting a little and respiratory depression can be an issue. Ketamine has a lot to recommend it but I have seen nasty dysphoria and that shouldn’t be dismissed. Dexmedetomidine has some strengths but there’s no doubt patients are sleepy for longer afterwards. Nitrous oxide clearly works but you do need a way of delivering it and you might not want it for too long in a tight space. Opioids obviously are superb for analgesia but require caution, particularly if used as an additive to another agent.
Again the key thing is to choose agents whose characteristics feel familiar to you and use them to manage the goals you came up with in the “why?” bit.
Is it just sedation you need. If it’s painful, how painful? Is that pain likely to be consistent or variable in nature? Does the time to wake matter? Would regional options help with those inputs?
Now choose the agent that lets you get things there.
Because a strange spot for sedation is really just a different office to do your work.
Here’s your patient. You can only just see some of the elements here, but the patient is covered up in blankets. They have earmuffs on. They have oxygen going and a cannula in place. After some midazolam, fentanyl and ketamine in we managed to sneak in digital nerve blocks. From that point on we really didn’t much of the ongoing infusion to have the patient snoozing but rousable to touch. The one obvious flaw here? We didn’t control the environment quite well enough to know the family had sent in a news reporter to get a shot.
And one hour in, with the patient relaxed we figured we might as well try a gentle pull on that hand. And it slid right out. Pity about the bath.
And all it needed was a bit of REST. Maybe that’s not so strange after all.
Notes:
It is very cool that you dropped by here. Remember that if you like the stuff we have on the site you can sign in for an email update when a new post goes up. Have a look around, it’s here somewhere.
Of course none of the posts are meant to be the final word. We’d love to learn from anyone if you have the time to leave a comment. No pressure though.
Yep I’ve had previous clearance to use this case in public.
The image of the job is as it appeared in the local paper, The Illawarra Mercury.
The other images are both from flickr in the Creative Commons area and are unchanged. The clown was posted by lorenzoclick and the sign came from Roadside Pictures.
Now have you scrolled all the way down here? Then I have a bit of a treat. In the presentation version I had a multi-exposure shot of Danny McCaskill in action in his film Cascadia. You could watch it by clicking here and reflect on safety. Or maybe just watch it because it’s amazing.
This is the written version of a talk by Dr Andrew Weatherall for the South African Society of Anesthesiologists Congress 2017, just held in Johannesburg. It’s probably just about the shiny things.
You probably figure that a talk on prehospital paediatric medicine in Sydney should be about shiny pictures of that thing we call the coat hanger. Or maybe actions shots of this character …
Morning BIF.
And of course there are a lot of cool things we can do in prehospital paediatric care. Maybe the best thing to do is to start with a story. It’s a story of a kid we’ll call B.
Lazy Mornings
One of the odd features of Sydney is that on its edges there are some areas that are essentially rural. They’d take an hour or so to drive to from the CBD, but are probably only 10-15 minutes flight from the base.
One day, a Monday I think, on one of the properties out that way there’s a Dad watching cartoons with a couple of his kids. They want to keep hanging out and he has a bit of work to do moving some earth so he heads out, kids parked firmly on the couch and closes the door behind him.
In the truck he starts to manoeuvre to turn it around. Back. Forward. Back with a glance at a side mirror and he sees legs. They look like the legs of his 4-year-old and they are sticking out from under the wheels.
I imagine the seconds it took to reach her felt like a long time. I imagine the wait for help to arrive felt a lot longer.
Things That Aren’t Common
The weird thing about being an Aussie talking about trauma in South Africa is that I am not talking about something that is common to us. Most of the audience would laugh at our numbers. The NSW Institute of Trauma and Injury Management published some stats from the 2015 annual review and across the whole of NSW there were 3970 major trauma patients. The busiest adult trauma centre would see a bit north of 600. Across the state the kids’ hospitals would see less than 200 severely injured kids between the three of them.
So I should pack up and stop talking I guess?
Well I guess the thing we could reflect on is that if you can’t rely on exposure to numbers to get everybody better and produce better outcomes there are other things you can focus on. You can start with the system to make the response bring the hospital to the patient quicker. It’s over an hours drive back once anyone gets there.
That day the NGO I spend time with was called about B and was airborne in minutes to get to her. This ability to get in the air quickly came from a trial to look at ways of getting care to patients quicker where every second that could be cut down was thrown in the bin.
The perpetual question we are asking is “what can we bring to the accident scene that will make things better?”
Change the Scene
Let’s imagine a different version for a minute. Let’s imagine in the perpetual construction site that seems to be outside most hospitals, this happened out the front door of where you work. What would you offer this kid?
My expectation is you’d rapidly assess for exsanguinating haemorrhage. You’d work as quickly as possible to ensure A, B and C are adequately sorted and you’d get analgesia on board. You’d image, transfuse if you need to, consider tranexamic acid and splint any fractures.
If oxygenation and ventilation means anaesthesia, intubation and ventilation (maybe even chest decompression) you’ll do that. You’ll assess and reassess as things evolve, operate where it’s really needed and keep making new plans to cope with a dynamic situation.
So here’s a question to consider – which one of these should we forget about while the patient travels by road for an hour to reach the front door of the hospital? If you’re the anaesthetist up in theatres who will meet them later, which ones do you not want to have been looked at early?
We can take almost anything we want to the scene. Helicopters carry stuff. So we take with us all the equipment for advanced airway management, a small ventilator and oxygen in our backpack. We can decompress chests. We can splint. We can ultrasound, tourniquet, pack wounds with haemostatic agents, give tranexamic acid and transfuse. We have to get there of course.
And on this day the team did. They were confronted with a child looking more than a bit pale and cool peripherally. Her HR was 140 and above with a brachial pulse palpable. Her GCS was 9/15. Her injuries were apparently below the umbilicus but looked like they included a fractured pelvis and right femur. She had been eviscerated and had a large skin flap extending from the front of the abdomen all the way around her back. She was still under the truck.
Over the next 50 minutes or so, the team obtained intraosseous then intravenous access. They performed a controlled rapid sequence intubation. They splinted fractures and covered up defects. They delivered warmed red cells. They got her to the hospital. She was fairly stable through the emergency department and then the operating theatres. She made it to PICU.
She made it home.
Cool story, huh? But also really irrelevant if you’re talking at a conference in a different health setting, right?
Another Change of Scene
What if this happened in Cape Town? Which team would turn up then. The dispatchers are likely not to have medical background. An activation of advanced teams will happen some time after the sent team gets there. The team that first arrives will have paramedics with variable levels of training. They might not be able to give a range of stronger analgesic agents. They will have more limited options for airway management. They are likely not to feel as comfortable with cannulation in kids as in adults.
The kid gets what they get.
The thing is, I could be describing the same back in Sydney. I gave you a story from the system on a good day. We know a system like that is there but we don’t really offer it. Most days our kids will get teams that finds kids really challenging (because they are of course).
Getting the Team There
How do I know this? Well we looked.
A while back CareFlight was running a randomised trial to try and activate advanced teams to patients on the basis of the initial information that gets called in using a strict protocol. The trial applied to adults but we were asked to offer it to kids as well.
The crew (doctor/paramedic/pilot/aircrew) next to the helicopter had access to the screens and took it in turns to match the high acuity calls to tasking criteria and even to call back for more info if required. A decision to get in the air, cross-checked with central coordination for kids) had to be made within about 5 minutes of the start of the call.
For a while the systems (crew watching and central coordination watching) operated alongside each other. So we had a look at how that worked out. Over a period of time where the Sydney area had 44 severely injured kids, on that initial info the advanced care crew picked up 20 of them. The central guys looking noticed 3.
The numbers are obviously small (not much trauma, remember) but when the crew were watching and going to jobs it also made differences to the system. As they always brought kids back to the kids’ trauma centre, the time to get there averaged 92 minutes. When they were not available (on another job or offline) that time became 296 minutes. That’s for a few reasons but in no small part to some of those patients getting taken to other hospitals and waiting for transfer.
So there’s one thing you can do for your more trained up teams without much infrastructure required to get the right team there.
And I hope someone picks it up because in Sydney they abandoned it. At the end of the trial the screens went.
Another Look
So we had another look to see if the system had picked up the slack. We looked at the time when the advanced crew had the screens and the time after that. These were longer time periods (34 months in the first epoch and 54 months after which equated to 71 severely injured kids before and 126 after).
In the first 34 months the collaborative system picked up 62% of those severely injured kids and the average time to hospital was 69 minutes. In that latter period, with centralised looking alone, 31% of kids were triaged to advanced care, the version of care the system says it wants. The time to reach the kids’ hospital averaged 97 minutes.
You can imagine that this is something I find … disappointing.
But you might also be thinking “If you are suggesting I try and change a whole system then you are an extremely crazy person affected by anaesthetic gases that have rotted your brain because that will involve meetings, and talking to people who do politics and some of those people will expect me to wear ties and that is not why I got into anaesthesia”.
And that is fair.
But a much as I’d love us to do things about systems there’s something we could all focus on right now to try and make a difference.
If the system is mostly going to send the “not pointy end” part of the system, then we should also look at the care most of the kids will receive.
The Big Story
Every talk on prehospital stuff by a doctor can end up being mostly about the really sharp edge. But in NSW less than 1 in 5 kids ever see the advanced care team. So the biggest bang for our buck is in making sure all the kids get access to prehospital clinicians who feel confident working with kids and give them what they need on indication, not influenced by age alone.
When we focus on the pointy end the chances for gains are pretty marginal. Let’s look at intubation for example. Advanced EMS practitioners in Switzerland have published on their efforts and the highly trained and experienced professionals mostly get the tube in without incident but almost 1 in 5 kids had the wrong-sized tube and the majority were placed too far down the airway. Bringing up the whole of the prehospital provider group to a level above Swiss advanced EMS is probably a pretty big effort.
Particularly when you look at stats like those from Prekker et al looking at a big EMS system in Washington where intubation was an option. A paeds response happens for them in 1 in 2198 callouts (there were 299 in total in 6 years spread across all the practitioners). Their first pass success was 66% (though they did eventually get there in 97%) and 10% of the patients needing intubation needed 3 or more attempts.
And I can’t tell you what the oxygenation was like through that and really oxygenation is the name of the game.
The simple truth is kids get a raw deal at the pointy end. Everyone finds them tougher. Bankole et al compared kids receiving high level EMS care around New Jersey with a severe traumatic brain injury and compared them to the adults being looked after by the same really well trained first responders.
20% of kids with a GCS under 8 had no attempt at airway intervention. Of those intubated 69.2% had complications and 29% (vs 2.27% in adults) had a failed intubation. Even cannulas were placed in only 65.7% vs 85.9%.
It starts making you think that if those of us in prehospital medicine looked harder at the thing we want to achieve, oxygenation, rather than interventions that sometimes can do that but have big potential complications we might be able to change things for a bigger population of kids.
Recalibration
Although there are problems drawing on battleground experience in civilian trauma care, particularly in kids, there is a quite interesting paper from Sokol et al. looking at the Camp Bastion experience with 766 kids with traumatic injuries. 20% of them needing some sort of intervention and circulation measures (particularly stopping bleeding) was the most effective. Simple airway manoeuvres were done not often enough and interventions for breathing (like chest decompression) were a lesser order issue than circulation issues.
So perhaps what we should focus are things we could train more people in and more prehospital providers of all experiences could deliver:
Recognising the sick kid.
Stopping haemorrhage effectively.
Assessing A and B and delivering effective bag-mask ventilation.
Cannulation and appropriate fluid use.
Recently we’ve done some focus group work at The Children’s Hospital at Westmead with clinicians who do paediatric airway management and one of the strong themes emerging as we write up is that all of them rate airway assessment and bag-mask ventilation as the most vital skill they want to be good at and they’d like to pass on.
There are all sorts of interesting hints here. Hansen et al conducted an exploratory study in 2016 to look at how well paramedics recognised and treated in croup. After whittling through records their small study looked at 14 patients with a primary upper airway issue. 8 of the patients had “stridor” or “croup” explicitly noted in the tasking or information noted by the responding paramedics. 6 had trigger words like “barky cough” or something pretty convincing. All of them received salbutamol, not the nebulised adrenaline or other treatments on offer.
But Some Things are Easy, Right?
Analgesia though, that might be an easier target because relieving pain in kid sis a no brainer.
Well, no.
Samuel et al. published a systematic review of evidence looking at analgesia provided by prehospital providers for kids in 2015. In it they describe a review of 55642 patients where 26% of the kids had trauma and another 16.1% of kids had a primary complaint with significant pain.
0.3% of the kids were given any analgesia.
There were other studies included reporting rates of analgesia administration for fractures of 2.1-3.2% (and at least one with 0% in the under 5s with fractures).
What is going on?
Well sometimes there might be limitations in what the paramedics have available (e.g. opioids or not, ketamine etc). One physician system showed 92% getting given strong analgesia in these sorts of patient groups.
There may be a fear of drug errors because there is work suggesting issues with drug dosing in kids in more than 30% of prehospital cases.
However Rahman et al have also done work exploring the perceptions of paramedics in providing analgesia to kids and showed very high levels of reported discomfort with providing and assessing analgesia in kids. More alarmingly 25% of respondents indicated that kids needed less analgesia because of immature nervous systems.
These are not small chips either. Schreier et al looked at PTSD symptoms after just mild to moderate trauma (things like isolated fractures) in kids. At 18 months (in an admittedly small study) 38% of the kids they looked at had at least mild symptoms.
PTSD in kids expresses itself as poor attendance at school, missed marks in education and social disengagement.
While < 4% of kids are getting analgesia for obviously painful things, there are things we can tackle that don’t need a rapid sequence intubation and a snorkel.
What is the cost?
So the cost to patients will undoubtedly be big if we are sending teams who don’t feel comfortable in kids, but is the cost of addressing it prohibitive.
I reckon not. Here’s one example.
CareFlight, that little charity I mentioned, has started to treat education of first responders as a way of providing service to the community. By taking simulation education and courses mobile to rural and remote first responders maybe we can make the first person who turns up to the injured just that little more comfortable that there are things they can do.
The MediSim crew in action next to a big red rock.
Since 2011 they’ve reached almost every state in Australia and trained more than 3000 people. Participants don’t pay.
In the Western Cape there is an EFAR program that would be worth checking out that is seeking to enhance the response of first-aid responders.
But if you’re an anaesthetist or other critical care provider, then there would have to be ways for you to link up with local prehospital services and offer to help paramedics gain skills and experience.
Everyone in the room (or reading this) can probably provide analgesia. Everyone has seen a sick kid. Everyone knows how to splint and work on stopping bleeding. In particular I am full of a room of people who have exquisite skills in things we think of as basic, like bag-mask ventilation, but could be the difference between a patient being oxygenated on the drive in, or obstructed the whole way.
The Wish List
If you’re the anaesthetist waiting in that operating theatre when an injured kid is on the way, what’s on your wish list?
Mine would include the patient being identified and getting to me as quickly as possible. I’d hope the team that reaches the patient can recognise if they’re sick and keep reassessing well. I’d hope they felt confident managing the airway and could optimise oxygenation as much as their skills allowed. I’d love it if they turned up with some form of intravascular access and some analgesia on board.
The priorities to start making that happen for more patients is actually not about BIF with the noisy rotors. The priorities are the same if you’re looking at an old bridge across a harbour. Or some mountain near the sea.
Or a downtown area closer to the sky.
Notes:
I cannot express the depth of my gratitude to the patient and family who have granted permission for the use of their story as part of education in this area.
Thanks also to the clinicians involved in the case, Dr Rob Bartolacci and Ben Southers, super paramedic, for background on their case and the shot from the sky that day.
A huge thanks also to the brilliant Jo Park-Ross, Flight Paramedic from AMS in Cape Town and Ross Hoffmeyr, an anaesthetist also working in this area down in Cape Town for helping me understand more about the local system and checking my work.
A shout out too to Colin Brown and Greg Brown (no relation) at CareFlight for the stuff about the MediSim program.
As part of the invited faculty the organising committee covered travel, accommodation and registration for the conference.
The images of BIF and Sydney are from my personal collection. Other images are from the Creative Commons area of flickr and are unmodified here. Paul Saad posted the shot of Johannesburg and the shot of Cape Town is by Damien du Toit.
So you’re out there somewhere and you really want to do a thing you think might help but you don’t have your standard kit. Can you adopt the lessons of Richard Dean Anderson and improvise? Mel Brown has you covered.
Okay, so I am guessing from the title of this post you have a good idea of my age….I am talking about the original MacGyver, not the new one. And for those of you that are too young to know who I am talking about…..MacGyver could improvise everything he ever needed from anything that was “just” lying around. I once saw him create an explosive device with little more than a pepper shaker and some foil wrapping off some chewing gum.
It is wonderful that we live in a world where most of the time we have access to all we need (and more), including our medical equipment. But what happens when you don’t have what you need (or don’t have enough of what you need) to treat your patient?
So in line with our series on “I wish I knew then what I know now” we are going to look at MacGyvering (improvising) arterial tourniquets and pelvic binders – two devices that we are all very familiar with (or if you’re not you can be if you go …
These easily reproducible techniques are certainly something I wish I knew about when I first started nursing…..and no, it wasn’t when Florence was around (although I am pretty sure she trained one of my lecturers).
Continuing with the History Theme
Did you know that arterial tourniquets have been around for a while now? In fact, the first combat commander to advocate the use of tourniquets was Alexander the Great – he based his decisions on the works of the medical researches at Cos.
However it wasn’t until 1718 that Louis Petit, a French Surgeon, developed a “screw device” that could be placed over blood vessels to stop flow. From the French verb “tourner” (to turn), he named the device “tourniquet.”
Elegant, non?
Improvised Arterial Tourniquets
One of the most important things to remember with any arterial tourniquet is that indirect pressure MUST be applied whilst the tourniquet is being applied. This will at least minimise if not stop the bleeding whilst the tourniquet is being applied…
Improvised tourniquets need to be at least 5cm wide to ensure adequate arterial occlusion can be achieved. Have you ever wondered why a shark attack victim that has had an improvised tourniquet applied to their bitten leg (usually via a surfboard leg rope) soon begins bleeding again after the bleeding was originally stopped? Well the theory goes that the initial narrow occlusion of the artery was enough to completely occlude the artery but as the pressure proximal to the point of occlusion builds up behind the narrow improvised tourniquet the arterial pressure is able to beat the tourniquet and the patient begins bleeding again. You need something applied over a wide area to get the job done.
So, what should we use? Firstly you need to find a windlass device that is thick enough and tough enough to withstand the pressure applied to it as you twist it to tighten the tourniquet (which can be up to 300mmHg of pressure). Some things (and only some, there would be more) that are readily available include:
A thick solid stick (not always ideal)
An indicator lever (probably not out of your own car)
A screwdriver
A tyre lever
A set of pliers
As for the tourniquet itself, what should be used? Some materials used with good effect include (but again are not limited to):
Triangular bandages (make sure these are the cotton ones and not the cheap paper ones)
Seatbelts (once again probably not out of your own car)
Canvas belts
Shirt sleeve (preferably with non-stretchy material)
Neck ties (not sure how many of these are around these days).
One of the issues with improvised tourniquets is the narrowing of the tourniquet at the windlass point. This can pinch the patient’s skin and make an already painful intervention more painful. The narrowing of the tourniquet material can also lead to greater damage to the underlying skin, muscles and nerves. Having said that I am not sure the alternative of death due to blood loss is ideal either.
I think many of us have spoken about how we could improvise an arterial tourniquet….but how do we actually do it? Let’s use the triangular bandage as our improvised tourniquet to discuss this in detail.
Ideally you want two triangular bandages – lay the first one along the arm or leg.
Wrap the second triangular bandage over the first and around the arm or leg and tie a knot or two.
Place the improvised windlass rod on top of the knot and tie two more knots to secure that windlass (note: if you can’t tie knots, tie lots).
Turn the windlass until the bleeding stops and then turn once more. Secure the windlass in place with the first triangular bandage.
If you forgot the first triangular bandage you can use gaffer tape (or equivalent) to secure the windlass in place.
It is important to still write “T” and the time of application somewhere obvious (maybe on the patient’s forehead would catch the eye) as you would for any arterial tourniquet. Obviously improvising is not ideal when compared to commercially available products. However, they are life saving for your patient when you don’t have the equipment that you need available.
Improvised Pelvic Binding
Improvised pelvic binding has been widely used throughout Australia by our Ambulance services for a very long time – I think most people would be familiar with pelvic sheeting. There’s some nuance around when pelvic binding may or may not be useful (just check out the posts here, here, here and here) but what do you do if you’ve made an assessment it is worth trying and you’re without your fancy gear?
Well we all go driving or hiking with sheets in our car boot (that’d be a trunk for our North American friends) or backpacks, right? I don’t think so, and I know I certainly don’t. So what do we commonly have on us that we could use? A jacket works well as an improvised pelvic binder. Let’s have a look at what this looks like:
Prepare the jacket for use. Use the arms as a width guide and fold it up like so.
Place the jacket under the smalls of the knees where there is a natural hollow.
Preferably with two operators seesaw the jacket up to the correct position over the greater trochanters.
Bring the arms of the jacket together and tie a knot.
Twist those sleeves until the required pressure is achieved.
Secure that knot (gaffer tape works again, or zip ties or equivalent).
You’re done. And maybe cold, but done.
Once again it is obvious that improvising is not ideal when compared to commercially available pelvic binders. However they are life saving for your patient when you don’t have the equipment that you need available. All interventions, whether improvised or not, must be continually checked for effectiveness – especially if your patient is moved.
Summary
It is important that as clinicians we understand how to use the commercially made equipment we have available to us. However, it is just as important that we know how to improvise life saving interventions as there will be a time when we won’t have our equipment (or enough of it) to treat our patients. This is a predicament that I certainly don’t want to find myself in. So let’s share what we know as shared knowledge is power. Or share what MacGyver knows because that is also power.
A bit more reading:
Those posts on arterial tourniquets and bleeding are here.
Sometimes it’s worth wondering if the things we hear, see and feel are quite as we thought they were. Dr Alan Garner has a look at your senses when you get into the chest and wonders whether it’s all as straight forward as we like to think?
Let’s start this post by stating right upfront that this is about chest wounds. If that is not what you were thinking then time to look elsewhere.
What I want to discuss is the clinical diagnosis of tension pneumothorax in the field. The reason for the discussion is that I believe it is way over-diagnosed. When I worked in the UK 6 years ago it seemed tension was being diagnosed frequently and the reason given was the sound as they breached the pleura with the forceps. As the patient was positive pressure ventilated at the time then the sound must have been air rushing out of the pleural space as their intrathoracic pressure was positive throughout the respiratory cycle right?
Remember how we can’t rely on the sounds involved in clinical examination in the prehospital environment because they’re too unreliable? Well I was being told this one was always right. ‘Always’ is a big word in medicine
I’m also aware of at least one case where a patient with a single epigastric gunshot wound from a low velocity weapon had intubation and then bilateral finger thoracostomies. The comment at the time was that the prehospital doctor, who no doubt went into it all in good faith, stated that at the time of the thoracostomies they found a pneumothorax on one side and a tension on the other.
However on imaging and surgery the projectile went straight back into the pancreas and nowhere near either hemithorax or the diaphragm. Indeed the only injuries identified to any part of the chest were the thoracostomy wounds themselves. Again an intubated patient so the intrathoracic pressure must have been positive right? If the lung felt down then it had to be a pneumothorax? And if there was a sound on breaching pleura it must have been a tension?
Clearly in the second case the signs were misleading so what is happening here? Let’s put aside for a second the challenges of the initial diagnosis of pneumothorax and focus on the feel with the finger and the sound to the ears. Could it be that some of the evidence we’ve been lead to believe tells us we’re dealing with a pneumothorax can mislead experienced, well trained clinicians?
Diving In
Perhaps I have done a few more chest drains than most. Partly that is due to more than 20 years in the prehospital space but I probably did even more when I was a registrar 25 year ago. I spent 6 months working for a couple of respiratory physicians and I put lots of drains (mainly for malignant effusions) in patients who certainly did not have a pneumothorax before I started. It was common to hear a noise as the pleura was breached as the air rushed in. But this of course was in spontaneously ventilating patients and that is different right?
Obviously we need to go back to the physiology to see what is driving the movement of air either into or out of the hole we have made to determine whether the sound we are hearing is air going in, or air going out.
Back to Basics
Transpulmonary pressure is the pressure gradient that drives normal ventilation. It is the difference between the alveolar pressure and the intrapleural pressure in the lungs.
Ptp = Palv – Pip. Where Ptp is transpulmonary pressure, Palv is alveolar pressure, and Pip is intrapleural pressure.
(If you’d like a little more on this the excellent Life in the Fast Lane has a bit on transpulmonary pressure here.)
Also it turns out that you can get a google preview of John West’s classic textbook on respiratory physiology. Take a moment to go and enjoy Figure 4-9 on page 59.
You can see from panel B (I meant it, go and have a look) that intrapleural pressure varies between about -5 and -8 cmH2O at the mid-lung level during normal respiration. It is always negative and that’s due to elastic recoil of the lung which is being opposed by the chest wall. It is less negative at the dependent regions of the lung (reducing alveolar size) and more negative at the apex (increasing alveolar size).
Let’s Add Air
In the situation of a small pneumothorax the air in the pleural space makes the intrapleural pressure less negative and the driving pressure difference for ventilation is therefore reduced. If the pneumothorax is completely open to the air such as with an open thoracostomy wound the intrapleural pressure is equal to atmospheric pressure, the elastic recoil of the lung causes complete collapse and ventilation by chest expansion is impossible – positive airway pressure has to be applied.
It is not the situation of the pneumothorax that particularly concerns me. If they are hypoxic or hypotensive and the patient has a pneumothorax the chest should be decompressed – a complete no-brainer. The question is why are good clinicians decompressing normal chests and thinking there was a pneumothorax or even a tension when there was not? Does the physiology lead us there?
Patient One
First let’s consider the non-intubated patient with normal respiration and no pneumothorax. This is the situation with the patients with malignant effusions I was putting drains in years ago. Here the alveolar pressure is never more than a cmH2O or two positive or negative. The intrapleural pressure however is -5 to -8 cmH2O. Therefore it does not matter what phase of respiration you breach the pleura, the pressure gradient between the pleural space and atmosphere is negative and air will rush in.
The gradient is bigger in inspiration when alveolar pressure is negative (and therefore the total pressure is around -8 cmH2O) and less negative during expiration when it is more like -5 cmH2O. It is however always negative. It does not matter which part of the respiratory cycle you breach the pleura, air is going to flow into the pleural space and the elastic recoil of the lung will drive it to collapse. If you hear a noise as I often did, it is air rushing in, the classic sucking chest wound. An iatrogenic one.
Patient Two
I don’t think anyone would have an issue with things so far. So let’s move on to the intubated patient who does not have a pneumothorax. I am going to assume here that there is not a lot of airway resistance in our trauma patient (which is not to say they don’t have underlying obstructive pulmonary disease, anaphylaxis to the induction drugs you gave or a clot sitting in a big bronchus/ETT) as it makes the discussion a bit easier to assume that resistance is minimal (futile according to the Daleks) and the pressure you are seeing on your ventilator gauge is largely transmitted directly to the alveoli.
Looking at our transpulmonary pressure equation, unless the airway pressure and hence alveolar pressure is higher than about 5 cmH2O then the gradient at the time you open the pleura means air is going to enter the pleural cavity. (If they have significant airway resistance this could happen with much higher airway pressures).
Just have a quick eyeball of this time pressure chart of a standard volume cycled ventilator with no PEEP (and a self-inflating bag will provide a similar though more variable trace). And I deliberately have no PEEP in this chart. PEEP is not likely to be the first thing we reach for in the hypotensive trauma patient we have just intubated where we are concerned about the possibility of a pneumothorax.
With normal lungs the peak pressure here is probably about 20 cmH2O. What proportion of the total respiratory cycle is the airway pressure (and hence the alveolar pressure in our patient with low airway resistance) likely to be below 5 cmH2O? If your little prehospital ventilator has a roughly 1:2 I:E ratio as most do, then the answer is most of it.
In other words unless you have PEEP of at least 5 cmH2O even in your intubated patient the transpulmonary pressure is negative for a good half of the respiratory cycle. During at least half the respiratory cycle, if you hear a noise as you breach the pleura you are hearing air rushing IN.
The elastic recoil of the lung is the reason that you feel the lung has collapsed by the time you pull the forceps out and put your finger in unless you have some PEEP in play.
Now I’m not saying there has never been a time when the air wasn’t rushing in. I don’t think much of the word “always” in medicine, remember? I’m just suggesting that what we know of physiology would argue that there is at least a solid proportion of the time where that transpulmonary pressure gradient is negative when you breach the pleura, which means that there’s likely to be a good proportion of cases where those “certain” clinical signs become less reliable.
For a demonstration of this with the mother of all open thoracotomies (in a cadaver) check out this video.
The cadaver is intubated, a “generous” pleural decompression wound has been created, and on each expiration the lung collapses right down unless PEEP is applied. And note the collapse is complete on each expiration.
As long as the thoracostomy is big enough to freely communicate with the air (and if you are relying on the open “finger” technique rather than putting in a drain it needs to be large or they may re-tension), when you put your finger in during expiration the lung will be collapsed unless there is a reasonable amount of PEEP splinting things open pretty impressively.
It will be collapsed whether it already was before you made the wound or whether it happened as you spread the forceps and made the communicating hole. The time between making the hole and getting that sense of lung up or lung down with the finger is ample time for the lung to collapse down. It seems like this particular clinical sign probably tells you nothing about the state of play prior to the wound being made.
So noises can be deceptive and feeling a collapsed lung just means that the lung recoiled as the pleura was opened. Can you even guarantee which phase of the respiratory cycle the patient was in when you made that hole? Unless you had at least 5 cmH2O (and maybe more) PEEP on at the time you breached the pleura neither of these signs necessarily means anything.
Maybe none of us can trust our big ears?
Now, what?
Again, I’m not really into saying things like “always” or “never”. What I’m suggesting is that there might be a lot more grey around these clinical signs than might first seem to be the case.
So how do you know if they had a pneumothorax? For me that is almost always by ultrasound now. I don’t know how I managed for 15 of those 20+ years of prehospital care without one. Sometimes of course the scan is equivocal and you need to make a call based on the signs you see and the condition of the patient but I find this to be very infrequent with a good high frequency linear probe.
And as for tension the hallmark is abnormal physiology, particularly blood pressure. If decompressing the chest fixes the physiology then they had a tension. If it does not then they had a simple pneumothorax – or none at all. Because the noise you heard as you breached the pleura may have been air either entering or leaving the building, hearing a noise does not help you either way. Was Elvis ever in the building at all?
Notes:
I had the brilliant Dr Blair Munford review a heap of the physiology here to make sure it matched up.
After that link to the LITFL bit on transpulmonary pressure again? Then go right here.
And John West’s masterpiece (well at least the page mentioned) is here.
That image of Nahni with the big ears was posted to the Creative Commons part of flickr by Allan Henderson and is unaltered here.
Oh, and in case you didn’t know the truly amazing John West, Adelaide boy made good, has recorded his whole lecture series for you to go and watch. Because when you’re in your 80s you’ll probably be contributing to medical education like that too, right?
Continuing a theme started with a practical post on direct and indirect pressure for haemorrhage control, Greg Brown (Education Manager amongst other things) discusses the things he’s learned about how to figure out what you need in a kit.
I remember the first time as a young Nursing Officer in the Australian Army I went on exercise (that’d be “manoeuvres” for you Americans, and “war games” for those that watch too many movies) and had to pack a medical kit. Not knowing what was required for the job (and not asking either) I had earlier visited the field pharmacy with a request that was essentially “one of everything you have, please Ma’am”.
The result? I spent three days being cold, wet, hungry and slow – the sheer size and weight of my medical kit meant that I had not enough room for “luxuries” such as a sleeping bag, raincoat or enough food.
Now what?
So, what has changed over the years? Well, I’d like to think that a lot has changed. Firstly, I now have the experience to know that if I cannot do my job (because of issues pertaining to cold / heat / hunger / thirst / ability to keep up etc) then I am a liability and not an asset. I have also learned that the greatest skill ANY prehospital care provider can possess is the ability to improvise. And finally, I’ve learned that big ticket “Hollywood” style medicine does not keep people alive but that, as a popular Australian breakfast cereal advertisement from the late 1980’s stated so eloquently, “the simple things in life are often the best”.
It is important to realise from the outset that there are arguably more variables in life when it comes to medical kits than there are medical conditions that need treating. Okay, that is a bit of an exaggeration, but hear me out. When creating a medical kit the individual must ask themselves a series of five questions that will guide the size, contents and capability of their kit.
Question 1: Who will be using the kit?
If the answer is simply yourself, then you can afford to consider taking items that are your favourite but not necessarily everybody else’s preferred option (caveat: they still need to be evidence based and supported by your clinical practice guidelines / protocols). An example is in regards to airways: you might be an avid supporter of the iGel whereas I sit firmly in the LMA Supreme camp whilst there also exist individuals who like the King-LT. One could argue that they all do similar things and possess commonalities (e.g. blind insertion, semi-secure airway etc) yet they each require necessary knowledge, skill and attitudes in order to make them work. The solution, in this case, is standardisation – not three separate but similar airway devices.
Question 2: What is the kit expected to be capable of doing?
Within CareFlight we have many different lines of operation; for ease lets call them Sydney, Darwin, International and Off-Shore. So, take our Sydney operation – CareFlight Rapid Response Helicopter (CRRH). CRRH works as part of a wider retrieval network to service the Sydney basin. The majority of its taskings are to traumas and near drownings, so its kit reflects this. CRRH is unlikely to be tasked to a ketoacidotic haemophiliac with sepsis on a background of COPD. Why? It services the Sydney basin where there are also around 50 ambulance stations, each staffed with well trained, well equipped and well-motivated paramedics who are standing by to deliver the patient to one of a dozen equally well staffed / trained / equipped / motivated hospitals, that are available 24/7. If CRRH is treating and transporting this patient then it is because they’ve been ejected off of their motorbike whilst completing stunts at the local motocross track (again, perhaps a slight exaggeration for this particular patient), so the activation is to a trauma. CRRH’s kit must reflect this, just as the Darwin, International and Off-Shore kits must (and do) reflect their demographics.
The same goes for medical kits of a more “tactical” nature. If your tactical kit (the one you wear on your rig when conducting a deliberate action / breach / clearance etc, or every day because you are clever and “that’s how you roll”) contains a laryngoscope then I’d respectfully suggest that you’ve got it all wrong. Interventions in this environment need to be high yield and rapidly applied whilst allowing for the maintenance of situational awareness. If you are head down / bum up intubating, you are not accounting for your own safety. Besides, is the expectation now that this patient will self-ventilate? Or does your tactical kit also contain a self-inflating bag or mechanical ventilator?
Question 3: How long does this kit need to last?
This is a question of stock holdings. When I think back to that first Army exercise in a medical role of mine I now ask myself “it was only three days long, so why did I need seven days’ supply of three different oral antibiotics – especially when we were within two hours walk of a field hospital?” My stock holdings were all wrong. Chatting with many others over the years (both military and civilian) I have found that this can be a common theme amongst pre-hospital care providers.
If some is good, more must be better, right? Wrong – more just means bigger, heavier and slower. Besides, if you brought it – you’re carrying it.
But what if one fails, won’t I need a second / third / fourth? To this I offer that if your plans are built around multiple failures in equipment then it is time to revisit your equipment list and look for alternatives that are more robust and reliable.
An important consideration when assessing how long your kit needs to last is: what is your mission? If your mission is to conduct humanitarian assistance in the wake of a natural disaster for a period of seven days then you are going to need a LOT of stuff – trust me, having deployed to a few natural disasters in my time you will require a very robust supply chain. But if your mission is to treat and transport one victim of that natural disaster at a time with a resupply between each mission then you don’t need that much gear. Besides, generally speaking the less you carry the faster (and further) you can travel.
Stock holdings are a balancing act. It is reasonable to build some redundancy into your medical kits (ever had that one vial of morphine in your kit smash when someone decided to use your kit as a stepladder?) but it must be balanced with the knowledge that if you brought it, you’re carrying it.
Question 4: Is the kit a “stand alone” or designed to be augmented?
Capability should be viewed in terms of three things:
people;
equipment; and
the ability to effectively combine the first two points.
I learned a long time ago that I was never going to be the only person in a group with medical training. Every “operator” (e.g. police officer, fire fighter, soldier, aircrew member, emergency service volunteer etc) has basic first aid training (and sometimes much more) and many will carry their own supply of essential items (i.e. arterial tourniquets, bandages, gloves etc). In situations where medical attention is required, medical personnel need to utilise the capabilities provided by others.
It is always worth considering this concept of capability when forming your plan; planning to combine medical kits in order to create improved capability is a useful concept. Most military and paramilitary units do just this; as an example, the Australian Army’s Parachute Surgical Team (PST; now superseded) built its equipment plans around the “what ifs” of war and how to ensure enough capability without carrying a whole hospital worth of equipment.
What do I mean by the “what ifs”? Well, I’m glad I asked myself this question.
What if the plane carrying the equipment got shot down before we could drop the stores? Well, each member of the PST parachuted with a medical kit that, when combined with those that others carried, formed an interim resuscitation and surgical suite. What if a paratrooper and his / her kit went missing? Well, there were just enough team members to space out on separate aircraft to create two identical suites. What if a paratrooper required more than first aid on the drop zone or during the advance? Well, each kit also contained the stores statistically required to treat a battle casualty.
Each kit creates a capability; but when combined they can provide so much more. This is an important concept to keep in mind when designing your medical kit.
It’s a bit like the Mighty Morphin Power Rangers. Individually they don’t necessarily get the job done but when combined they offer … Spandex. And also getting things done.
Question 5: Can you actually carry it?
Size matters. I’ve said it a few times already, but size really does matter – if you brought it, you’re carrying it.
For a medical kit to be effective it needs to be capable of getting to and travelling with the patient. Therefore, if it is so big and cumbersome (because you packed one of everything…and some redundancy) that you cannot get to the patient then you need to ask yourself “what is the point?”.
Now, I will freely acknowledge that different sizes are required for different tasks – in fact, I have four different kits in my personal armoury for four different purposes. Similarly, CareFlight has different sized kits for different tasks within its separate lines of operation.
So some things to consider include:
Is this kit staying in a vehicle (if so, what type of vehicle?) or does it need to be portable by an individual?
If it is portable, what else is that person carrying (e.g. a tactical kit will likely sit between other pouches / holsters on a belt or chest rig whereas a bigger kit may come with shoulder straps or need to fit inside another pack)?
When packing it, how many pouches will you need to open in order to perform one intervention? (Note: the answer should be one; if your IV cannula, sterile wipe, venous tourniquet, securing tapes, bung, giving set and fluids are not together then you’ve got it wrong.)
OK I may have a bit of a kit fetish but each one has a specific purpose in life. Beyond just making me happy even.
Summary
So there you have it. Added to the list of “things I know now that I wish I knew then” is medical kits. I now start with an analysis of the mission, draw out the likely tasks, consider the need for redundancy, look at what else I need to carry and consider the overall capability. What I don’t do is request “one of everything please, Ma’am”.
Notes:
This one is much more of a recount of personal experience so there aren’t a heap of links to send you to. It would be great if people could give examples of how they think about their kits and what they carry though. It’s a good bet there are clever people out there who would point out things that haven’t come up here.
Oh, and don’t forget if you like the stuff on here there should be a spot somewhere on the page that lets you follow along so you’ll get an email when a post goes up.